

Prevalence and severity of corona virus disease 2019 (COVID-19): A systematic review and meta-analysis
- PMID: 32315817
- PMCID: PMC7195434
- DOI: 10.1016/j.jcv.2020.104371
Prevalence and severity of corona virus disease 2019 (COVID-19): A systematic review and meta-analysis
Abstract
Background: Since being first reported in Wuhan, China, in December 8, 2019, the outbreak of the novel coronavirus, now known as COVID-19, has spread globally. Some case studies regarding the characteristics and outcome of patients with COVID-19 have been published recently. We conducted a meta-analysis to evaluate the risk factors of COVID-19.
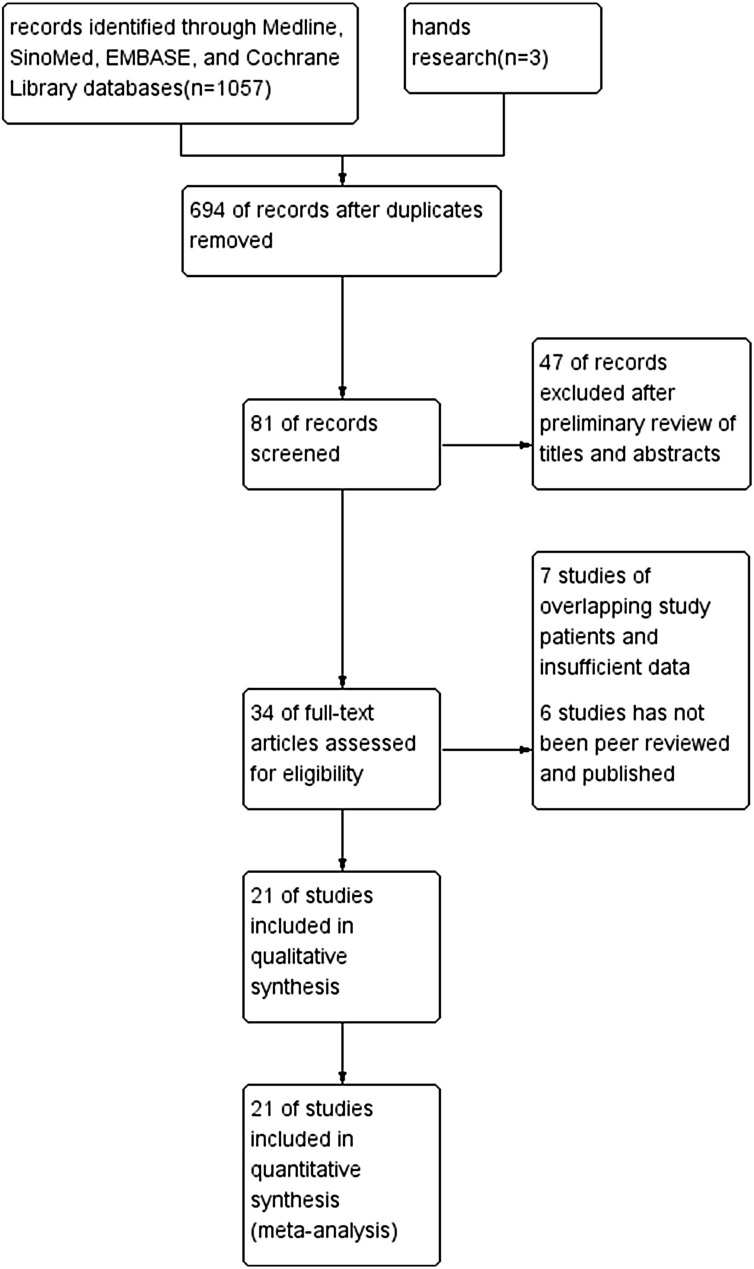
Methods: Medline, SinoMed, EMBASE, and Cochrane Library were searched for clinical and epidemiological studies on confirmed cases of COVID-19.
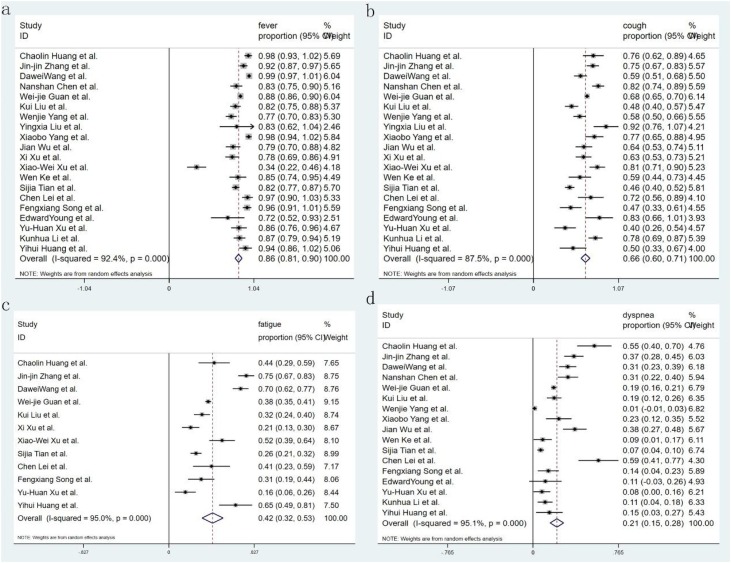
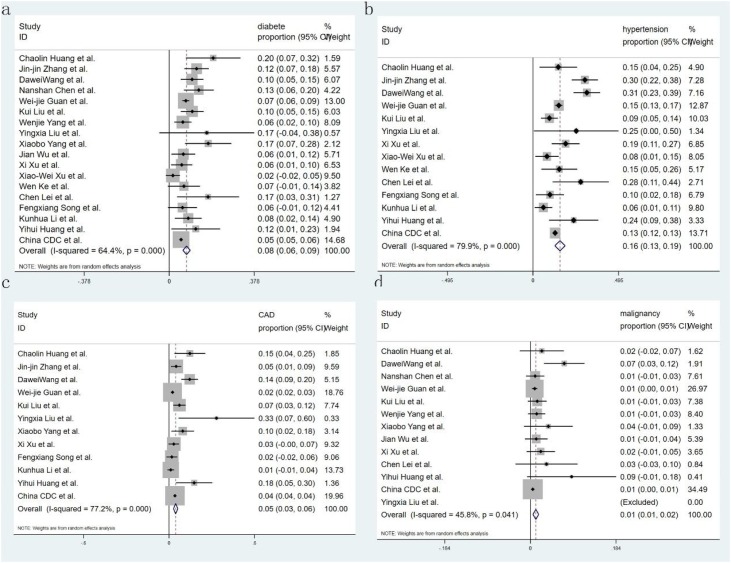
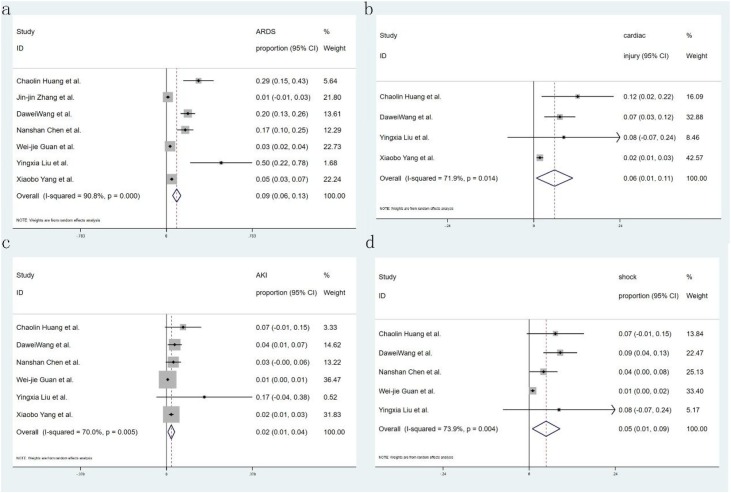
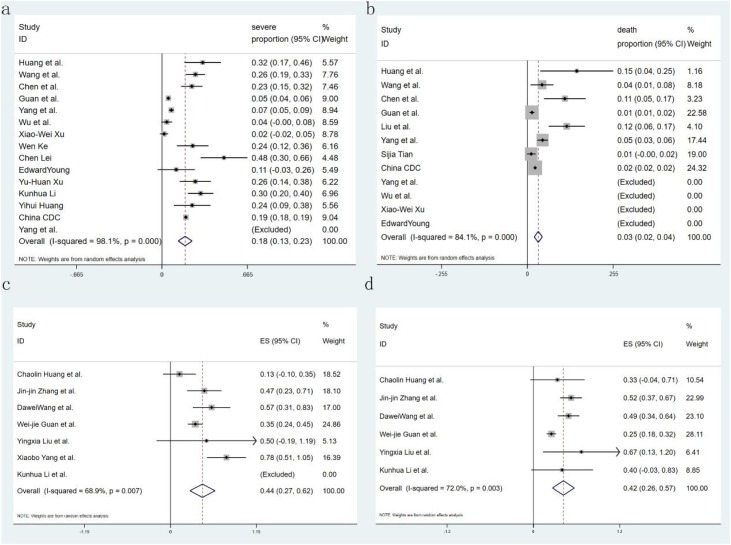
Results: The incidence of fever, cough, fatigue, and dyspnea symptoms were 85.6 % (95CI 81.3-89.9 %), 65.7 % (95CI 60.1-71.4 %), 42.4 % (95CI 32.2-52.6 %) and 21.4 % (95CI 15.3-27.5 %). The prevalence of diabetes was 7.7 % (95CI 6.1-9.3 %), hypertension was 15.6 % (95CI 12.6-18.6 %), cardiovascular disease was 4.7 % (95CI 3.1-6.2 %), and malignancy was 1.2 % (95CI 0.5-1.8 %). The complications, including ARDS risk, ranged from 5.6-13.2 %, with the pooled estimate of ARDS risk at 9.4 %, ACI at 5.8 % (95CI 0.7-10.8 %), AKI at 2.1 % (95CI 0.6-3.7 %), and shock at 4.7 % (95CI 0.9-8.6 %). The risks of severity and mortality ranged from 12.6 to 23.5% and from 2.0 to 4.4 %, with pooled estimates at 18.0 and 3.2 %, respectively. The percentage of critical cases in diabetes and hypertension was 44.5 % (95CI 27.0-61.9 %) and 41.7 % (95CI 26.4-56.9 %), respectively.
Conclusion: Fever is the most common symptom in patients with COVID-19. The most prevalent comorbidities are hypertension and diabetes which are associated with the severity of COVID-19. ARDS and ACI may be the main obstacles for patients to treatment recovery. The case severe rate and mortality is lower than that of SARS and MERS.
Keywords: COVID-19; Comorbidities; Mortality; Severity; Symptom.
Copyright © 2020 Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Comment in
-
Issues for conducting meta-analyses in COVID-19. Commentary on "Prevalence and severity of corona virus disease 2019 (COVID-19): A systematic review and meta-analysis''.J Clin Virol. 2020 Jul;128:104389. doi: 10.1016/j.jcv.2020.104389. Epub 2020 Apr 28. J Clin Virol. 2020. PMID: 32387969 Free PMC article. No abstract available.
-
Case fatality rate in patients with COVID-19 infection and its relationship with length of follow up.J Clin Virol. 2020 Jul;128:104415. doi: 10.1016/j.jcv.2020.104415. Epub 2020 May 5. J Clin Virol. 2020. PMID: 32403011 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
