

Modification of Muscle-Related Hormones in Women with Obesity: Potential Impact on Bone Metabolism
- PMID: 32316563
- PMCID: PMC7230770
- DOI: 10.3390/jcm9041150
Modification of Muscle-Related Hormones in Women with Obesity: Potential Impact on Bone Metabolism
Abstract
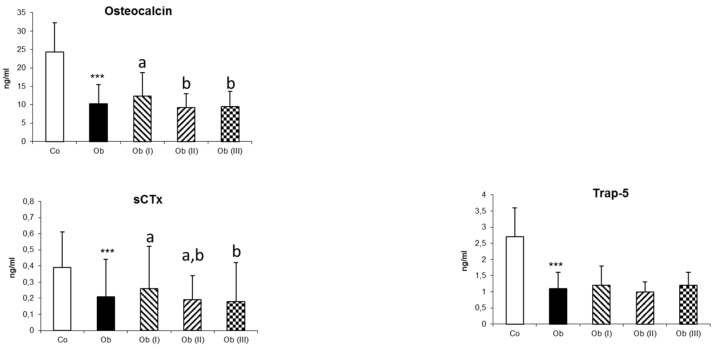
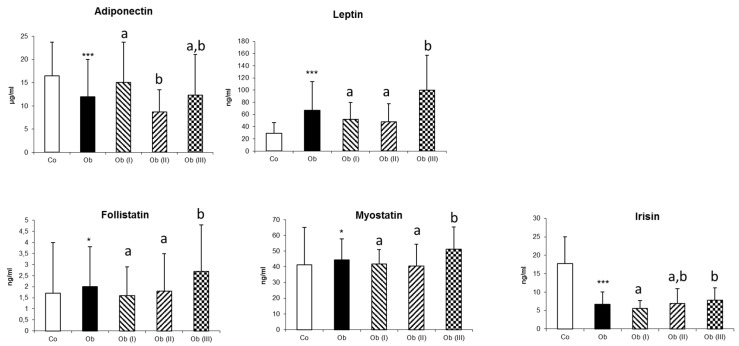
Lean body mass (LBM) is a determinant of areal bone mineral density (aBMD) through its mechanical actions and quite possibly through its endocrine functions. The threefold aims of this study are: to determine the effects of obesity (OB) on aBMD and myokines; to examine the potential link between myokines and bone parameters; and to determine whether the effects of LBM on aBMD are mediated by myokines. aBMD and myokine levels were evaluated in relation to the body mass index (BMI) in 179 women. Compared with normal-weight controls (CON; n = 40), women with OB (n = 139) presented higher aBMD, myostatin and follistatin levels and lower irisin levels. Except for irisin levels, all differences between the OB and CON groups were accentuated with increasing BMI. For the whole population (n = 179), weight, BMI, fat mass (FM) and LBM were positively correlated with aBMD at all bone sites, while log irisin were negatively correlated. The proportion of the LBM effect on aBMD was partially mediated (from 14.8% to 29.8%), by log irisin, but not by follistatin or myosin. This study showed that myokine levels were greatly influenced by obesity. However, irisin excepted, myokines do not seem to mediate the effect of LBM on bone tissue.
Keywords: areal bone mineral density; bone remodelling markers; myokines; obesity.
Conflict of interest statement
I certify that neither I nor my co-authors have a conflict of interest as described above that is relevant to the subject matter or materials included in this work.
Figures
References
-
- Sornay-Rendu E., Boutroy S., Vilayphiou N., Claustrat B., Chapurlat R.D. In obese postmenopausal women, bone microarchitecture and strength are not commensurate to greater body weight: The Os des Femmes de Lyon (OFELY) study. J. Bone Miner. Res. 2013;28:1679–1687. doi: 10.1002/jbmr.1880. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
