

Brain-heart interaction after acute ischemic stroke
- PMID: 32317013
- PMCID: PMC7175494
- DOI: 10.1186/s13054-020-02885-8
Brain-heart interaction after acute ischemic stroke
Abstract
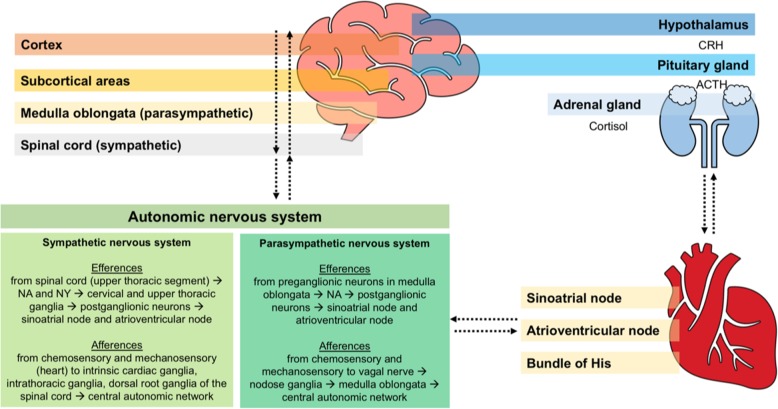
Early detection of cardiovascular dysfunctions directly caused by acute ischemic stroke (AIS) has become paramount. Researchers now generally agree on the existence of a bidirectional interaction between the brain and the heart. In support of this theory, AIS patients are extremely vulnerable to severe cardiac complications. Sympathetic hyperactivity, hypothalamic-pituitary-adrenal axis, the immune and inflammatory responses, and gut dysbiosis have been identified as the main pathological mechanisms involved in brain-heart axis dysregulation after AIS. Moreover, evidence has confirmed that the main causes of mortality after AIS include heart attack, congestive heart failure, hemodynamic instability, left ventricular systolic dysfunction, diastolic dysfunction, arrhythmias, electrocardiographic anomalies, and cardiac arrest, all of which are more or less associated with poor outcomes and death. Therefore, intensive care unit admission with continuous hemodynamic monitoring has been proposed as the standard of care for AIS patients at high risk for developing cardiovascular complications. Recent trials have also investigated possible therapies to prevent secondary cardiovascular accidents after AIS. Labetalol, nicardipine, and nitroprusside have been recommended for the control of hypertension during AIS, while beta blockers have been suggested both for preventing chronic remodeling and for treating arrhythmias. Additionally, electrolytic imbalances should be considered, and abnormal rhythms must be treated. Nevertheless, therapeutic targets remain challenging, and further investigations might be essential to complete this complex multi-disciplinary puzzle. This review aims to highlight the pathophysiological mechanisms implicated in the interaction between the brain and the heart and their clinical consequences in AIS patients, as well as to provide specific recommendations for cardiovascular management after AIS.
Keywords: Acute ischemic stroke; Arrhythmia; Cardiovascular; Cerebrovascular; Heart; Neuroinflammation.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures





References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
