

Efficacy of erector spinae plane block for postoperative analgesia in total mastectomy and axillary clearance: A randomized controlled trial
- PMID: 32317873
- PMCID: PMC7164476
- DOI: 10.4103/sja.SJA_625_19
Efficacy of erector spinae plane block for postoperative analgesia in total mastectomy and axillary clearance: A randomized controlled trial
Abstract
Background: The erector spinae plane block is a newer technique of analgesia to the chest wall.
Objective: The study was carried out to establish the efficacy and safety of this block in patients undergoing total mastectomy and axillary clearance.
Design: Prospective randomized controlled study.
Setting: Single tertiary care center, the study was conducted over a period of 1 year.
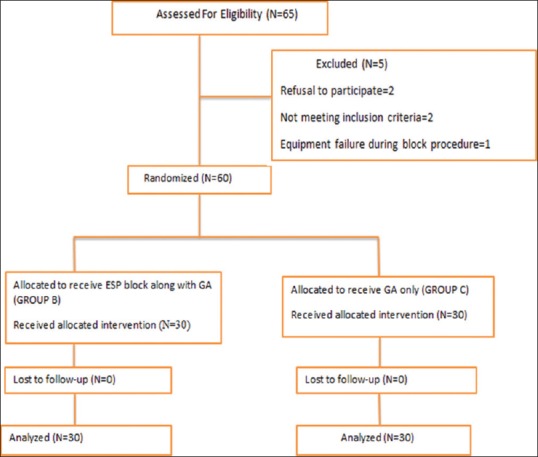
Patients: 65 patients were included; final analysis was done for 60 female patients undergoing total mastectomy and axillary clearance under general anesthesia were randomly allocated to two groups.
Intervention: Group B (block group) received ultrasound-guided erector spinae plane block at T5 level with ropivacaine (0.5%, 0.4 mL/kg) while the control group did not receive any intervention. Postoperatively, patients in both groups received morphine via intravenous patient-controlled analgesia device. Patients were followed up for 24 h postoperatively.
Main outcome measures: The 24-hour morphine consumption was considered as the primary outcome and secondary outcomes included time to first rescue analgesia, pain scores at 0, ½, 1, 2, 4, 6, 8, 12, and 24 h and characteristics and complications associated with block procedure.
Results: The 24-hour morphine consumption was 42% lower in block group compared to control group [mean (SD), 2.9 (2.5) mg vs 5.0 (2.1) mg in group B and group C, respectively, P = 0.01]. The postoperative pain score was lower in group B vs group C at 0, 1/2, 1, 2, 4, 6, 12, and 24 h (P < 0.05). 26 patients in group C against 14 in group B used rescue analgesia within 1 h of surgery (P = 0.01).
Conclusion: Erector spinae block may prove to be a safe and reliable technique of analgesia for breast surgery. Further studies comparing this technique with other regional techniques are required to identify the most appropriate technique.
Keywords: Acute postoperative pain; analgesia; breast surgery; erector spinae plane block; pain score; patient-controlled; regional anesthesia; ropivacaine; total mastectomy and axillary clearance; ultrasound-guided.
Copyright: © 2020 Saudi Journal of Anesthesia.
Conflict of interest statement
There are no conflicts of interest.
Figures

References
-
- Carpenter JS, Andrykowski MA, Sloan P, Cunningham L, Cordova MJ, Studts JL, et al. Postmastectomy/post lumpectomy pain in breast cancer survivors. J Clin Epidemiol. 1998;51:1285–92. - PubMed
-
- Cheng GS, Ilfeld BM. A review of postoperative analgesia for breast cancer surgery. Pain Manag. 2016;6:603–18. - PubMed
-
- Vila H, Liu J, Kavasmaneck D. Paravertebral block: New benefits from an old procedure. Curr Opin Anaesthesiol. 2007;20:316–8. - PubMed
-
- Chakraborty A, Khemka R, Datta T, Mitra S. COMBIPECS, the single-injection technique of pectoral nerve blocks 1 and 2: A case series. J Clin Anesth. 2016;35:365–8. - PubMed
LinkOut - more resources
Full Text Sources
Medical