

Epidemiology and Clinical Management of Fusarium keratitis in the Netherlands, 2005-2016
- PMID: 32318355
- PMCID: PMC7146074
- DOI: 10.3389/fcimb.2020.00133
Epidemiology and Clinical Management of Fusarium keratitis in the Netherlands, 2005-2016
Abstract
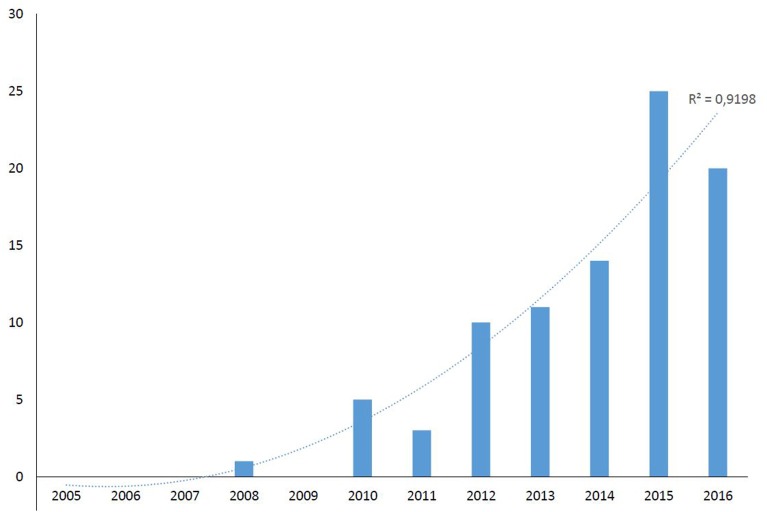
Introduction: Recognizing fungal keratitis based on the clinical presentation is challenging. Topical therapy may be initiated with antibacterial agents and corticosteroids, thus delaying the fungal diagnosis. As a consequence, the fungal infection may progress ultimately leading to more severe infection and blindness. We noticed an increase of fungal keratitis cases in the Netherlands, especially caused by Fusarium species, which prompted us to conduct a retrospective cohort study, aiming to describe the epidemiology, clinical management, and outcome. Materials and Methods: As fungi are commonly sent to the Dutch mycology reference laboratory for identification and in vitro susceptibility testing, the fungal culture collection was searched for Fusarium isolates from corneal scrapings, corneal swabs, and from contact lens (CL) fluid, between 2005 and 2016. All Fusarium isolates had been identified up to species level through sequencing of the ITS1-5.8S-ITS2 region of the rDNA and TEF1 gene. Antifungal susceptibility testing was performed according to the EUCAST microbroth dilution reference method. Antifungal agents tested included amphotericin B, voriconazole, and natamycin. In addition, susceptibility to the antisepticum chlorhexidine was tested. Ophthalmologists were approached to provide demographic and clinical data of patients identified through a positive culture. Results: Between 2005 and 2016, 89 cases of Fusarium keratitis from 16 different hospitals were identified. The number of cases of Fusarium keratitis showed a significant increase over time (R2 = 0.9199), with one case in the first 5 years (2005-2009) and multiple cases from 2010 and onwards. The male to female ratio was 1:3 (p = 0.014). Voriconazole was the most frequently used antifungal agent, but treatment strategies differed greatly between cases including five patients that were treated with chlorhexidine 0.02% monotherapy. Keratitis management was not successful in 27 (30%) patients, with 20 (22%) patients requiring corneal transplantation and seven (8%) requiring enucleation or evisceration. The mean visual acuity (VA) was moderately impaired with a logMAR of 0.8 (95% CI 0.6-1, Snellen equivalent 0.16) at the time of Fusarium culture. Final average VA was within the range of normal vision [logMAR 0.2 (95% CI 0.1-0.3), Snellen equivalent 0.63]. CL wear was reported in 92.9% of patients with Fusarium keratitis. The time between start of symptoms and diagnosis of fungal keratitis was significantly longer in patients with poor outcome as opposed to those with (partially) restored vision; 22 vs. 15 days, respectively (mean, p = 0.024). Enucleation/evisceration occurred in patients with delayed fungal diagnosis of more than 14 days after initial presentation of symptoms. The most frequently isolated species was F. oxysporum (24.7%) followed by F. solani sensu stricto (18%) and F. petroliphilum (9%). The lowest MICs were obtained with amphotericin B followed by natamycin, voriconazole, and chlorhexidine. Conclusion: Although Fusarium keratitis remains a rare complication of CL wear, we found a significant increase of cases in the Netherlands. The course of infection may be severe and fungal diagnosis was often delayed. Antifungal treatment strategies varied widely and the treatment failure rate was high, requiring transplantation or even enucleation. Our study underscores the need for systematic surveillance of fungal keratitis and a consensus management protocol.
Keywords: Fusarium; chlorhexidine; contact lenses; fungal keratitis; identification; susceptibility; visual outcome.
Copyright © 2020 Oliveira dos Santos, Kolwijck, van Rooij, Stoutenbeek, Visser, Cheng, Santana, Verweij and Eggink.
Figures
References
-
- Arendrup M. C., Guinea J., Cuenca-Estrella M., Meletiadis J., Mouton J. W., Lagrou K., et al. (2015). Method for the Determination of Broth Dilution Minimum Inhibitory Concentrations of Antifungal Agents for Conidia Forming Moulds. EUCAST. - PubMed
-
- Bruggink J. W. (2013). Ruim 6 op de 10 mensen dragen een bril of contactlenzen (Over 6 out of 10 people wear glasses or contact lenses). Centraal Bureau voor de Statistiek, Den Haag/Heerlen.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials