

Klotho protein contributes to cardioprotection during ischaemia/reperfusion injury
- PMID: 32319182
- PMCID: PMC7294144
- DOI: 10.1111/jcmm.15293
Klotho protein contributes to cardioprotection during ischaemia/reperfusion injury
Abstract
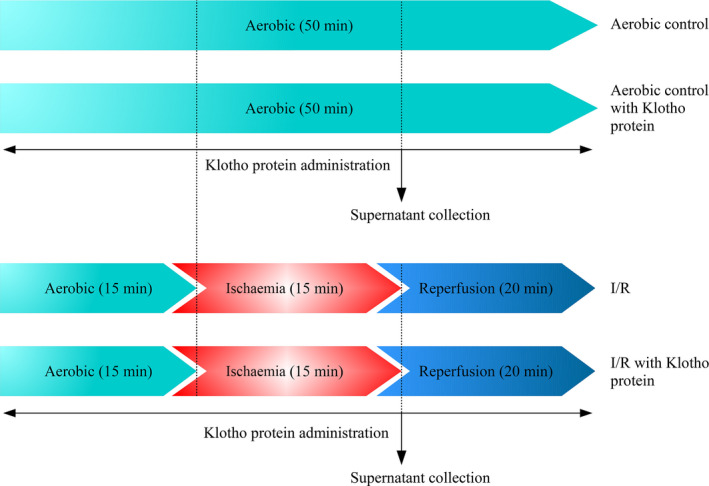
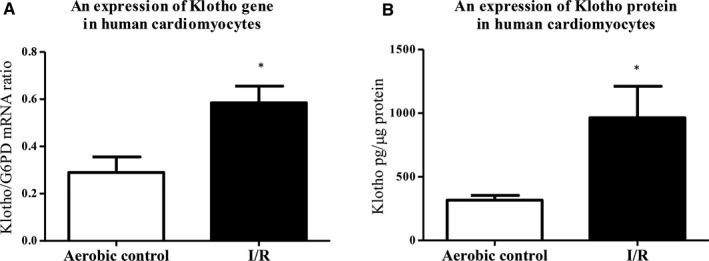
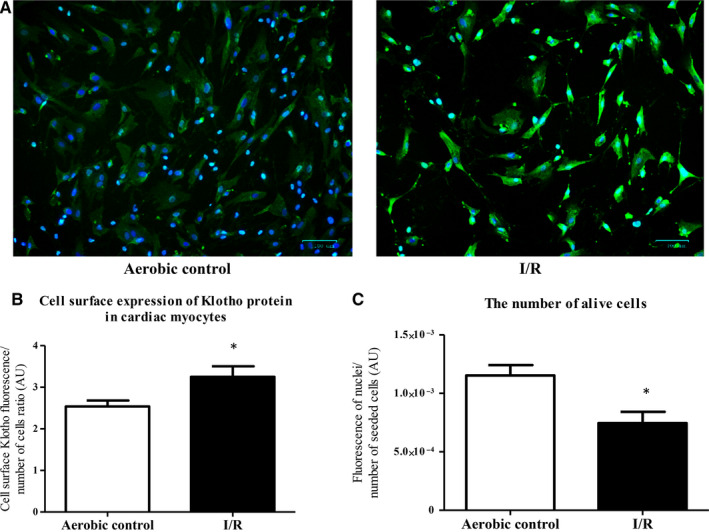
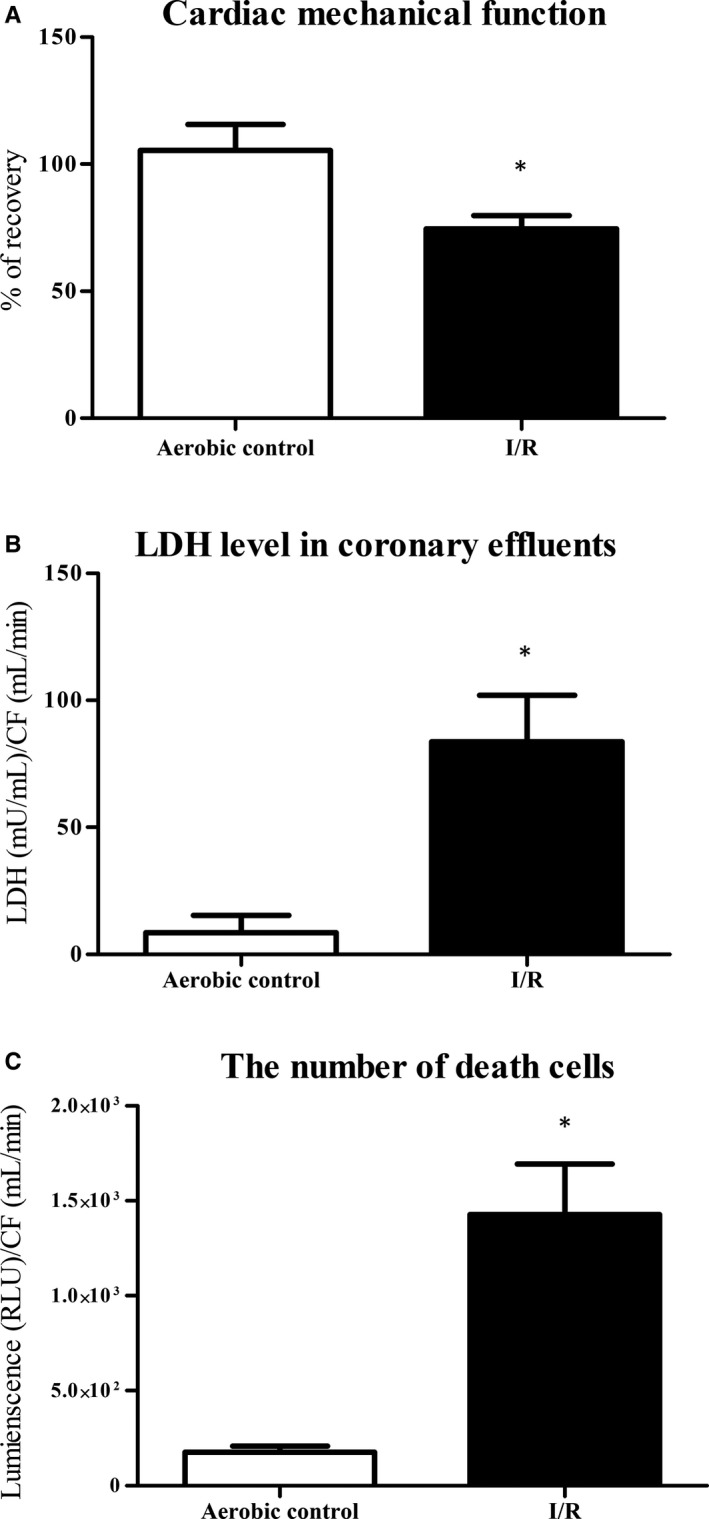
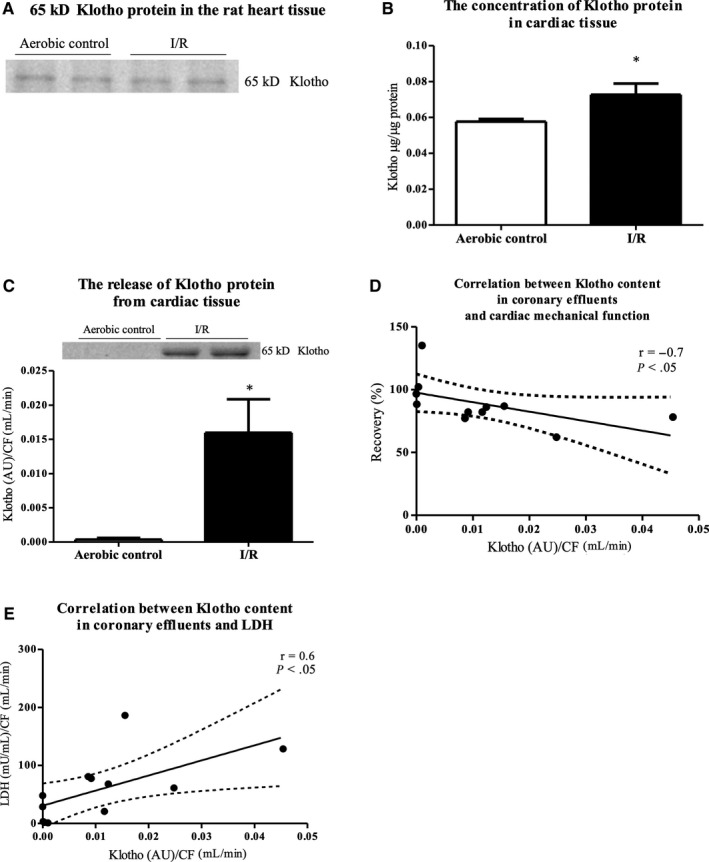
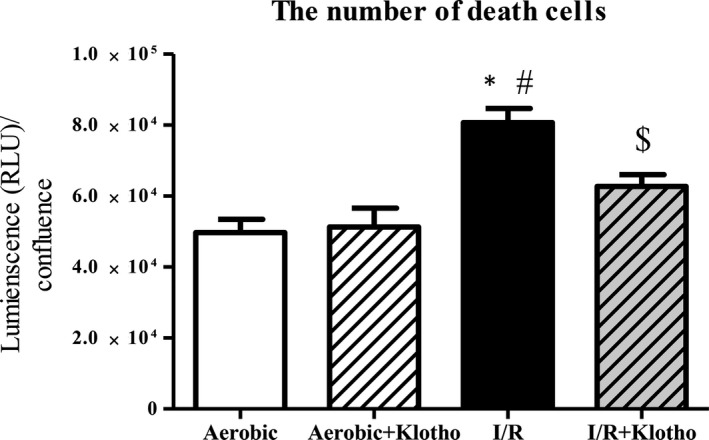
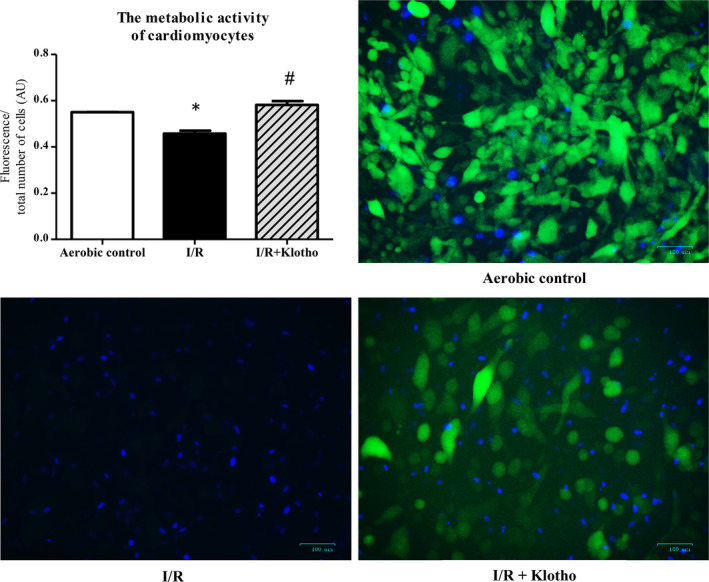
Restoration of blood flow to ischaemic heart inflicts ischaemia/reperfusion (I/R) injury, which manifests in metabolic and morphological disorders. Klotho is a protein with antioxidative and antiapoptotic activity, and is involved in the regulation of inflammation and fibrosis. The aim of the current research was to determine the role of Klotho in the heart subjected to I/R injury, as well as to study Klotho as a potential cardioprotective agent. Human cardiomyocytes and Wistar rat hearts perfused using Langendorff method subjected to I/R have been used. Hemodynamic parameters of heart function, markers of I/R injury, and gene and protein expression of Klotho were measured. Human cardiomyocytes were also incubated in the presence of recombinant Klotho protein, and the viability of cells was measured. There was a higher expression of Klotho gene and protein synthesis in the cardiomyocytes subjected to I/R injury. The compensatory production and release of Klotho protein from cardiac tissue during I/R were also shown. The treatment of cardiomyocytes subjected to I/R with Klotho protein resulted in increased viability and metabolic activity of cells. Thus, Klotho contributes to compensatory mechanism during I/R, and could be used as a marker of injury and as a potential cardiopreventive/cardioprotective agent.
Keywords: Klotho protein; cardiac markers; cardioprotection; ischaemia/reperfusion injury.
© 2020 The Authors. Journal of Cellular and Molecular Medicine published by Foundation for Cellular and Molecular Medicine and John Wiley & Sons Ltd.
Conflict of interest statement
The authors confirm that there are no conflicts of interest.
Figures
References
-
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST‐elevation myocardial infarction—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction). Circulation. 2004;110:588‐636. - PubMed
-
- Heusch G, Gersh BJ. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: a continual challenge. Eur Heart J. 2017;38:774‐784. - PubMed
-
- Zhao Z‐Q, Vinten‐Johansen J. Postconditioning: reduction of reperfusion‐induced injury. Cardiovasc Res. 2006;70:200‐211. - PubMed
-
- Tsutsui H, Kinugawa S, Matsushima S. Oxidative stress and heart failure. Am J Physiol Heart Circ Physiol. 2011;301:H2181‐H2190. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
