

Off-label Use of Direct Oral Anticoagulants Compared With Warfarin for Left Ventricular Thrombi
- PMID: 32320043
- PMCID: PMC7177639
- DOI: 10.1001/jamacardio.2020.0652
Off-label Use of Direct Oral Anticoagulants Compared With Warfarin for Left Ventricular Thrombi
Abstract
Importance: Left ventricular (LV) thrombi can arise in patients with ischemic and nonischemic cardiomyopathies. Anticoagulation is thought to reduce the risk of stroke or systemic embolism (SSE), but there are no high-quality data on the effectiveness of direct oral anticoagulants (DOACs) for this indication.
Objective: To compare the outcomes associated with DOAC use and warfarin use for the treatment of LV thrombi.
Design, setting, and participants: A cohort study was performed at 3 tertiary care academic medical centers among 514 eligible patients with echocardiographically diagnosed LV thrombi between October 1, 2013, and March 31, 2019. Follow-up was performed through the end of the study period.
Exposures: Type and duration of anticoagulant use.
Main outcomes and measures: Clinically apparent SSE.
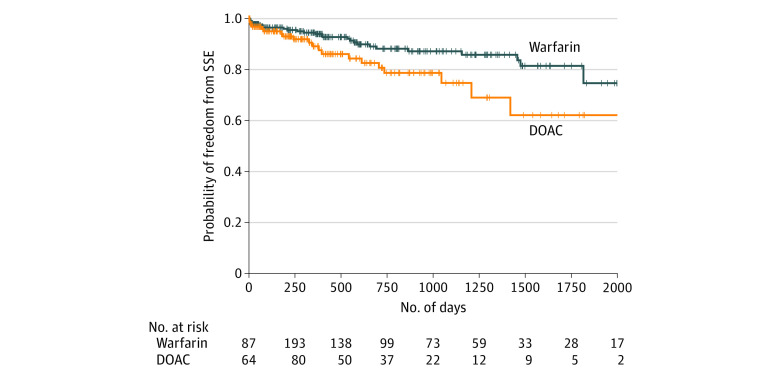
Results: A total of 514 patients (379 men; mean [SD] age, 58.4 [14.8] years) with LV thrombi were identified, including 300 who received warfarin and 185 who received a DOAC (64 patients switched treatment between these groups). The median follow-up across the patient cohort was 351 days (interquartile range, 51-866 days). On unadjusted analysis, DOAC treatment vs warfarin use (hazard ratio [HR], 2.71; 95% CI, 1.31-5.57; P = .01) and prior SSE (HR, 2.13; 95% CI, 1.22-3.72; P = .01) were associated with SSE. On multivariable analysis, anticoagulation with DOAC vs warfarin (HR, 2.64; 95% CI, 1.28-5.43; P = .01) and prior SSE (HR, 2.07; 95% CI, 1.17-3.66; P = .01) remained significantly associated with SSE.
Conclusions and relevance: In this multicenter cohort study of anticoagulation strategies for LV thrombi, DOAC treatment was associated with a higher risk of SSE compared with warfarin use, even after adjustment for other factors. These results challenge the assumption of DOAC equivalence with warfarin for LV thrombi and highlight the need for prospective randomized clinical trials to determine the most effective treatment strategies for LV thrombi.
Conflict of interest statement
Figures

Comment in
-
High Rates of Off-label Prescribing and the Urgent Need for a Randomized Clinical Trial.JAMA Cardiol. 2020 Jun 1;5(6):692-693. doi: 10.1001/jamacardio.2020.0612. JAMA Cardiol. 2020. PMID: 32319997 No abstract available.
-
To DOAC or Not to DOAC for Left Ventricular Thrombi-What Is the Dose?JAMA Cardiol. 2021 May 1;6(5):603-604. doi: 10.1001/jamacardio.2020.6894. JAMA Cardiol. 2021. PMID: 33471023 No abstract available.
-
To DOAC or Not to DOAC for Left Ventricular Thrombi-What Is the Dose?-Reply.JAMA Cardiol. 2021 May 1;6(5):604. doi: 10.1001/jamacardio.2020.6897. JAMA Cardiol. 2021. PMID: 33471031 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
