

Surgical and regional treatments for colorectal cancer metastases in older patients: A systematic review and meta-analysis
- PMID: 32320417
- PMCID: PMC7176093
- DOI: 10.1371/journal.pone.0230914
Surgical and regional treatments for colorectal cancer metastases in older patients: A systematic review and meta-analysis
Erratum in
-
Correction: Surgical and regional treatments for colorectal cancer metastases in older patients: A systematic review and meta-analysis.PLoS One. 2021 Apr 27;16(4):e0251005. doi: 10.1371/journal.pone.0251005. eCollection 2021. PLoS One. 2021. PMID: 33905447 Free PMC article.
Abstract
Objective: The present study explored the existing literature to describe the outcomes of surgical and regional treatments for colorectal cancer metastases (mCRC) in older patients.
Methods: A literature search was conducted in PubMed, EMBASE, Cochrane and ClinicalTrials.gov for studies published since 2000 that investigated the short- and long-term outcomes of regional treatments (surgical or non-surgical) for mCRC in patients aged ≥65 years. Pooled data analyses were conducted by calculating the risk ratio (RR), mean differences (MD) and hazard ratio (HR) between older and younger patients or between two different approaches in older patients.
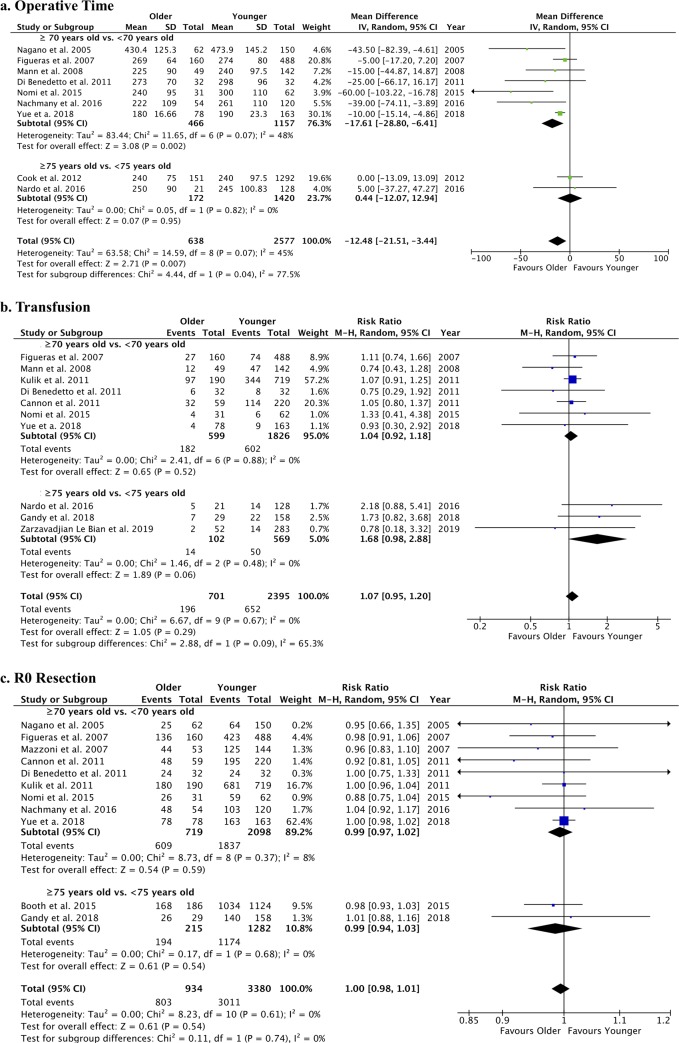
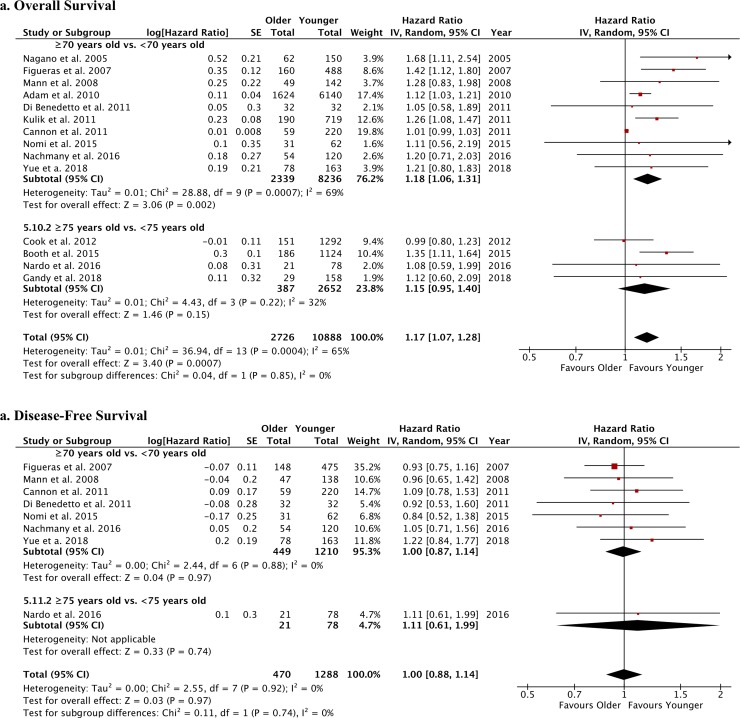
Results: After screening 266 articles, 29 were included in this review. These studies reported the outcomes of surgery (n = 19) and non-surgical local ablation treatments (n = 3) for CRC metastases in older vs. younger patients or compared the outcomes of different interventions in older patients (n = 7). When comparing older vs. younger patients undergoing liver surgery for mCRC, pooled data analysis showed higher postoperative mortality [RR = 2.53 (95%CI: 2.00-3.21)] and shorter overall survival [HR = 1.17 (95%CI: 1.07-1.18)] in older patients, whereas no differences in operative outcomes, postoperative complications and disease-free survival were found. When comparing laparoscopy vs. open surgery for liver resection in older mCRC patients, laparoscopy was associated with fewer postoperative complications [RR = 0.27 (95%CI: 0.10-0.73)].
Conclusion: Liver resection for mCRC should not be disregarded a priori in older patients, who show similar operative and postoperative outcomes as younger patients. However, clinicians should consider that they are at increased risk of postoperative mortality and have a worse overall survival, which may reflect comorbidities and frailty.
Conflict of interest statement
Pr P Pessaux is an orator for Integra and a co-founder of VirtualiSurg. This affiliation does not alter our adherence to PLOS ONE policies on sharing data and materials. All other authors have nothing to disclose, and all authors have declared that no competing interests exist in relation to the matter of this study.
Figures



References
-
- (WHO) WHO. Global Health and Aging. In: Aging NIo, Health NIo, Services UDoHaH, editors. 2011.
-
- Foreman KJ, Marquez N, Dolgert A, Fukutaki K, Fullman N, McGaughey M, et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories. Lancet. 2018;392(10159):2052–90. 10.1016/S0140-6736(18)31694-5 - DOI - PMC - PubMed
-
- Ganz PA. Does (or should) chronologic age influence the choice of cancer treatment? Oncology (Williston Park). 1992;6(2 Suppl):45–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
