

Metagenomics Reveals a Core Macrolide Resistome Related to Microbiota in Chronic Respiratory Disease
- PMID: 32320621
- PMCID: PMC7397787
- DOI: 10.1164/rccm.201911-2202OC
Metagenomics Reveals a Core Macrolide Resistome Related to Microbiota in Chronic Respiratory Disease
Abstract
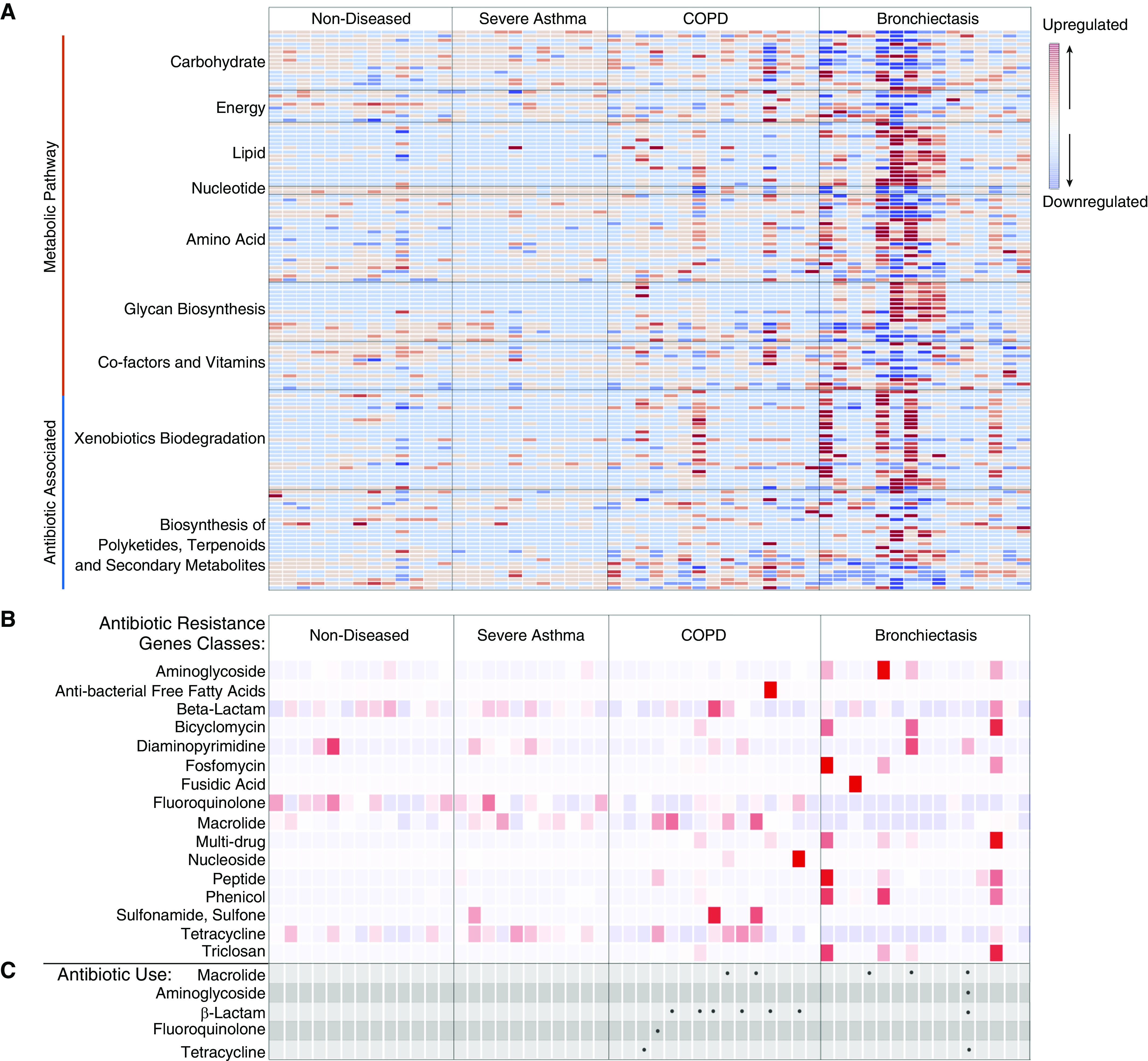
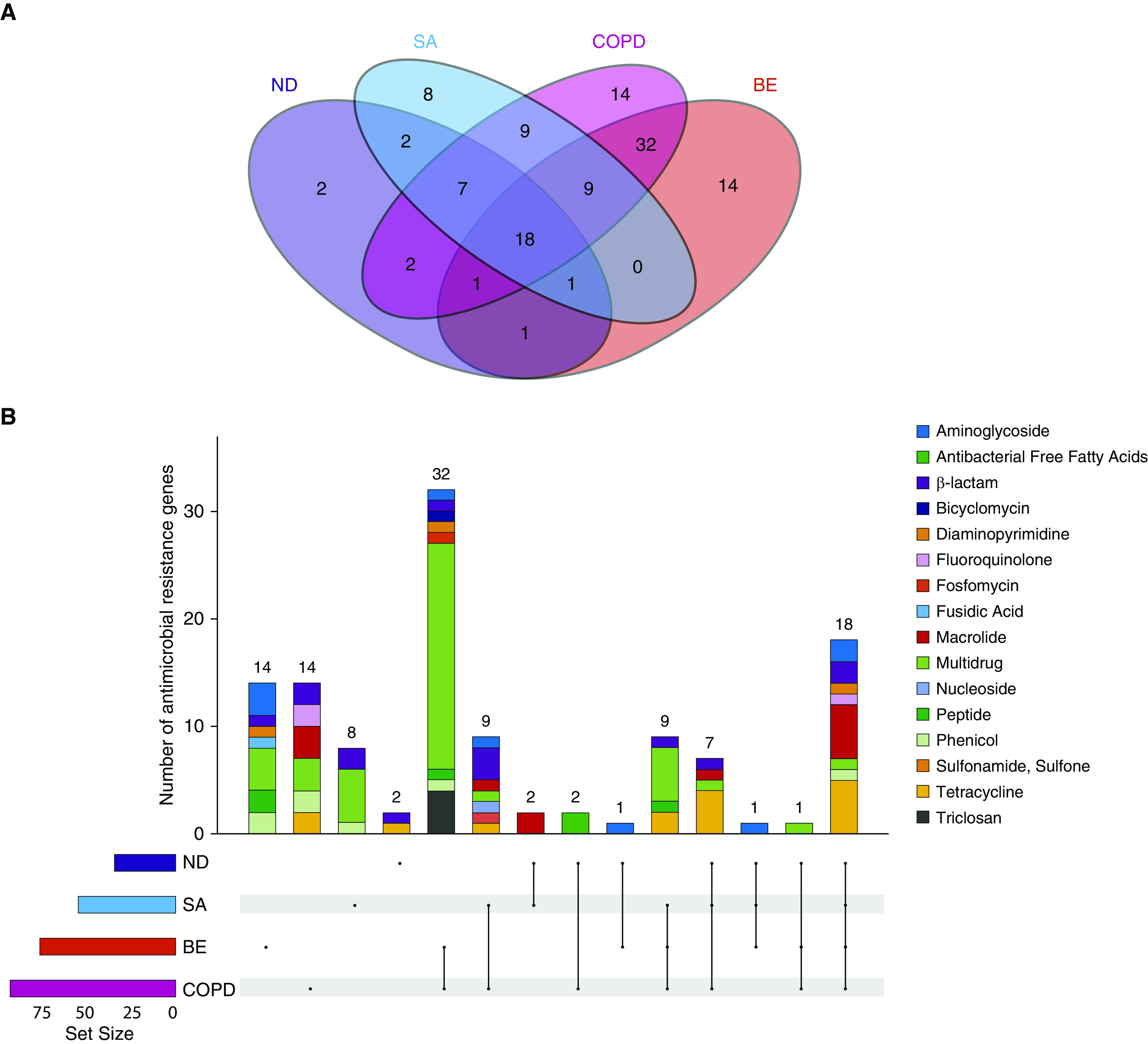
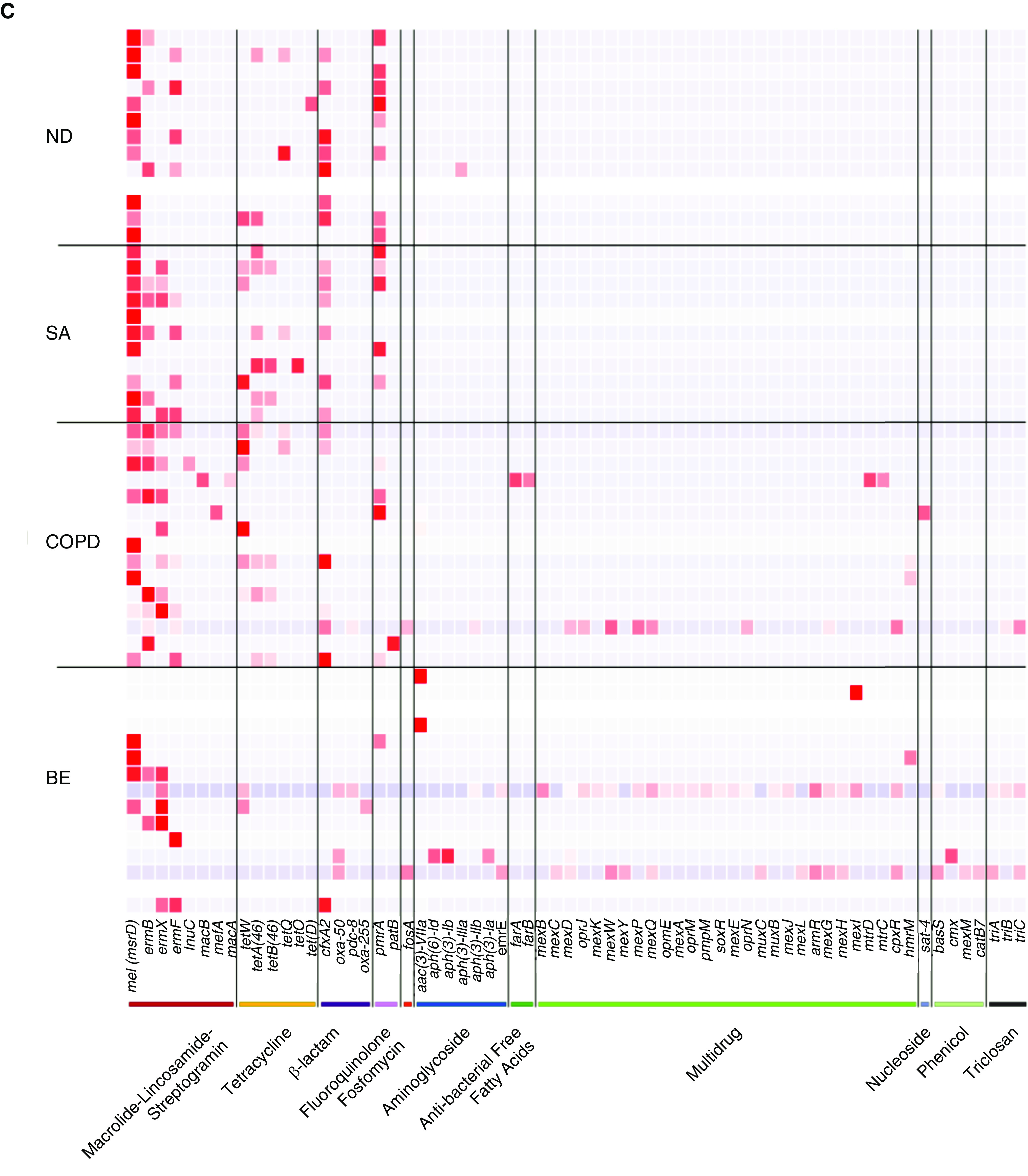
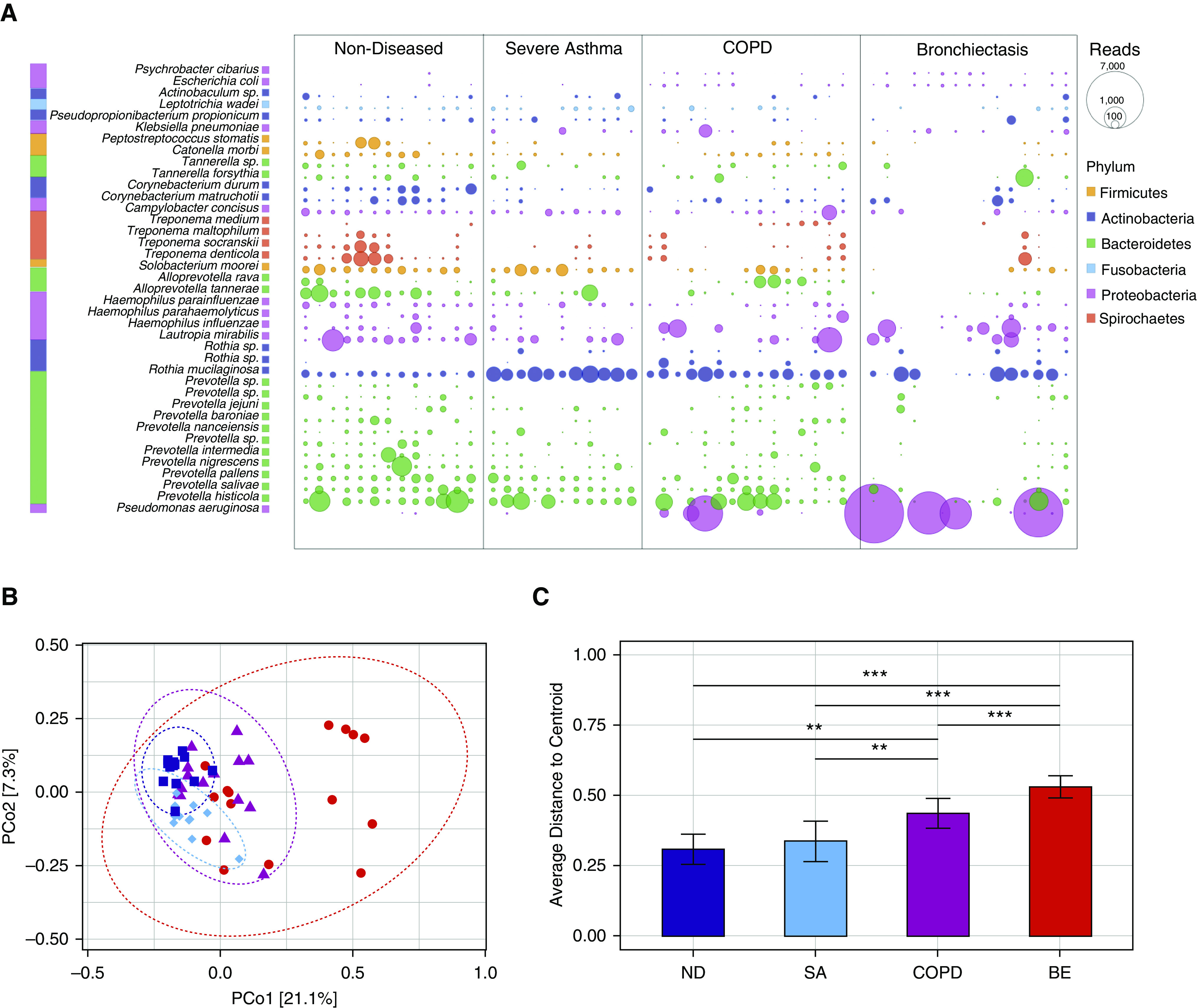
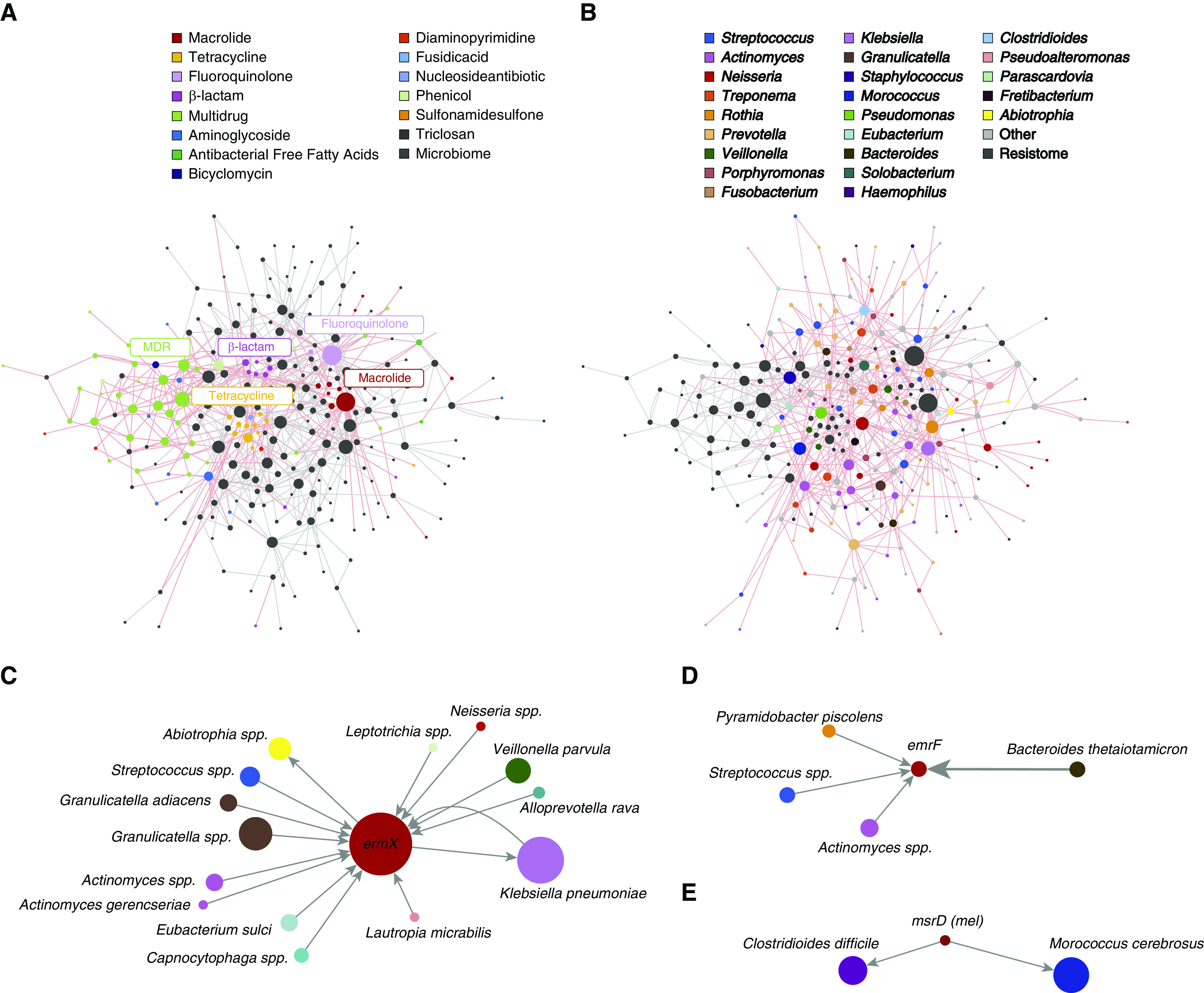
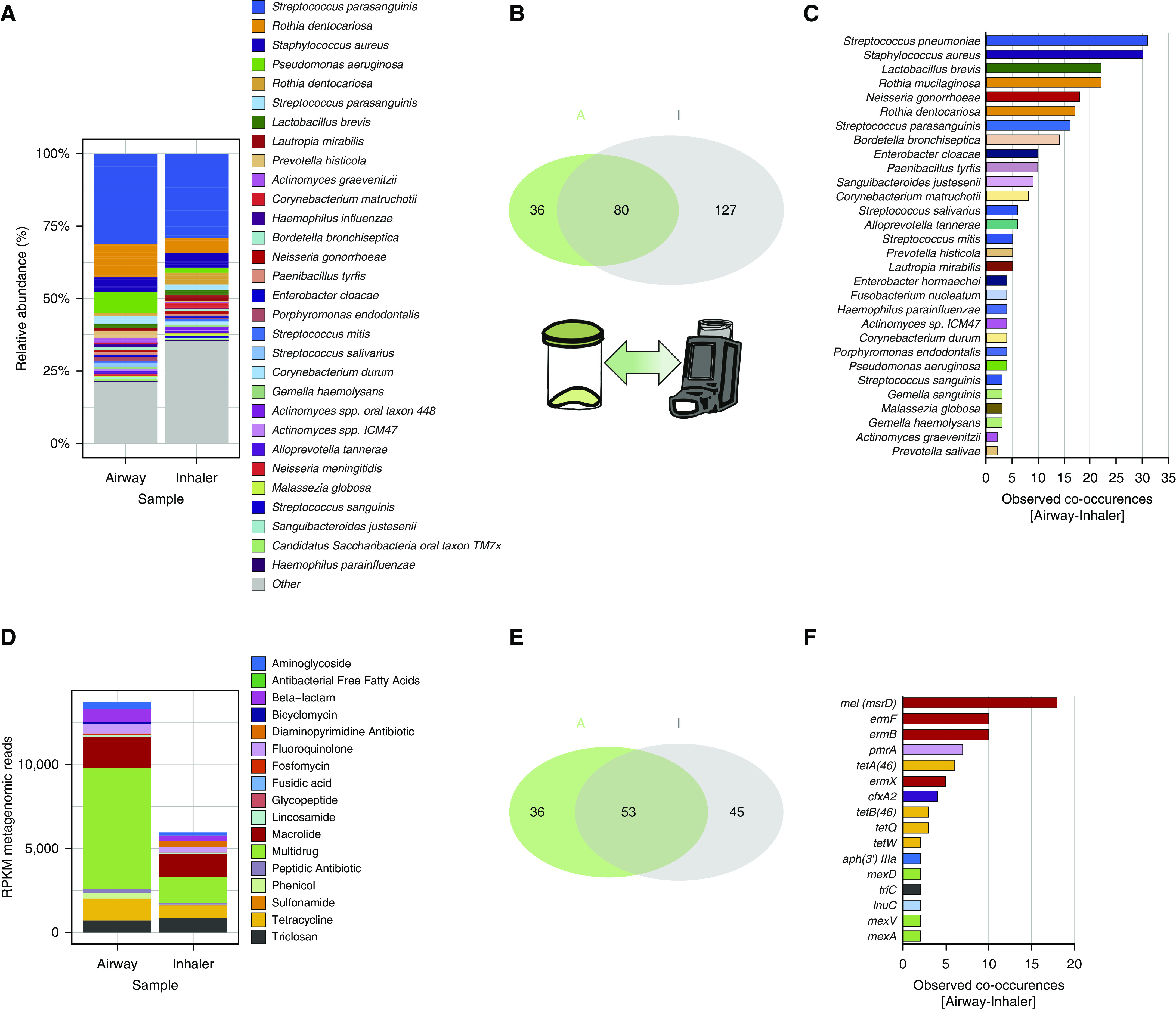
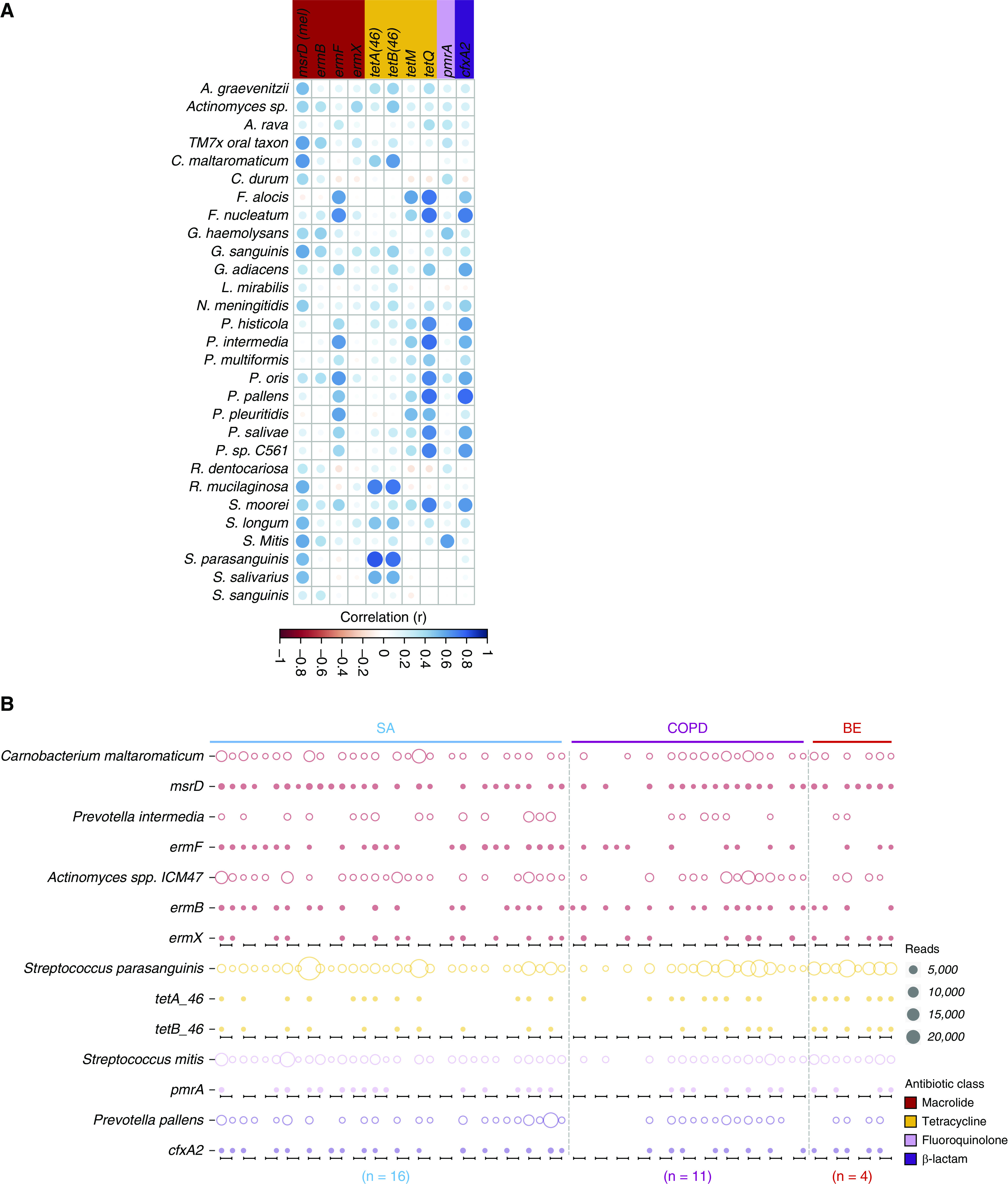
Rationale: Long-term antibiotic use for managing chronic respiratory disease is increasing; however, the role of the airway resistome and its relationship to host microbiomes remains unknown.Objectives: To evaluate airway resistomes and relate them to host and environmental microbiomes using ultradeep metagenomic shotgun sequencing.Methods: Airway specimens from 85 individuals with and without chronic respiratory disease (severe asthma, chronic obstructive pulmonary disease, and bronchiectasis) were subjected to metagenomic sequencing to an average depth exceeding 20 million reads. Respiratory and device-associated microbiomes were evaluated on the basis of taxonomical classification and functional annotation including the Comprehensive Antibiotic Resistance Database to determine airway resistomes. Co-occurrence networks of gene-microbe association were constructed to determine potential microbial sources of the airway resistome. Paired patient-inhaler metagenomes were compared (n = 31) to assess for the presence of airway-environment overlap in microbiomes and/or resistomes.Measurements and Main Results: Airway metagenomes exhibit taxonomic and metabolic diversity and distinct antimicrobial resistance patterns. A "core" airway resistome dominated by macrolide but with high prevalence of β-lactam, fluoroquinolone, and tetracycline resistance genes exists and is independent of disease status or antibiotic exposure. Streptococcus and Actinomyces are key potential microbial reservoirs of macrolide resistance including the ermX, ermF, and msrD genes. Significant patient-inhaler overlap in airway microbiomes and their resistomes is identified where the latter may be a proxy for airway microbiome assessment in chronic respiratory disease.Conclusions: Metagenomic analysis of the airway reveals a core macrolide resistome harbored by the host microbiome.
Keywords: antimicrobial resistance; macrolides; metagenomics; resistome; respiratory disease.
Figures
Comment in
-
Metagenomic Characterization of the Respiratory Microbiome. A Pièce de Résistance.Am J Respir Crit Care Med. 2020 Aug 1;202(3):321-322. doi: 10.1164/rccm.202005-1686ED. Am J Respir Crit Care Med. 2020. PMID: 32442018 Free PMC article. No abstract available.
References
-
- Sibila O, Laserna E, Shoemark A, Keir HR, Finch S, Rodrigo-Troyano A, et al. Airway bacterial load and inhaled antibiotic response in bronchiectasis. Am J Respir Crit Care Med. 2019;200:33–41. - PubMed
-
- Miravitlles M, Anzueto A. Antibiotics for acute and chronic respiratory infection in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;188:1052–1057. - PubMed
