

Human TH1 and TH2 cells targeting rhinovirus and allergen coordinately promote allergic asthma
- PMID: 32320734
- PMCID: PMC7483727
- DOI: 10.1016/j.jaci.2020.03.037
Human TH1 and TH2 cells targeting rhinovirus and allergen coordinately promote allergic asthma
Abstract
Background: Allergic asthmatic subjects are uniquely susceptible to acute wheezing episodes provoked by rhinovirus. However, the underlying immune mechanisms and interaction between rhinovirus and allergy remain enigmatic, and current paradigms are controversial.
Objective: We sought to perform a comprehensive analysis of type 1 and type 2 innate and adaptive responses in allergic asthmatic subjects infected with rhinovirus.
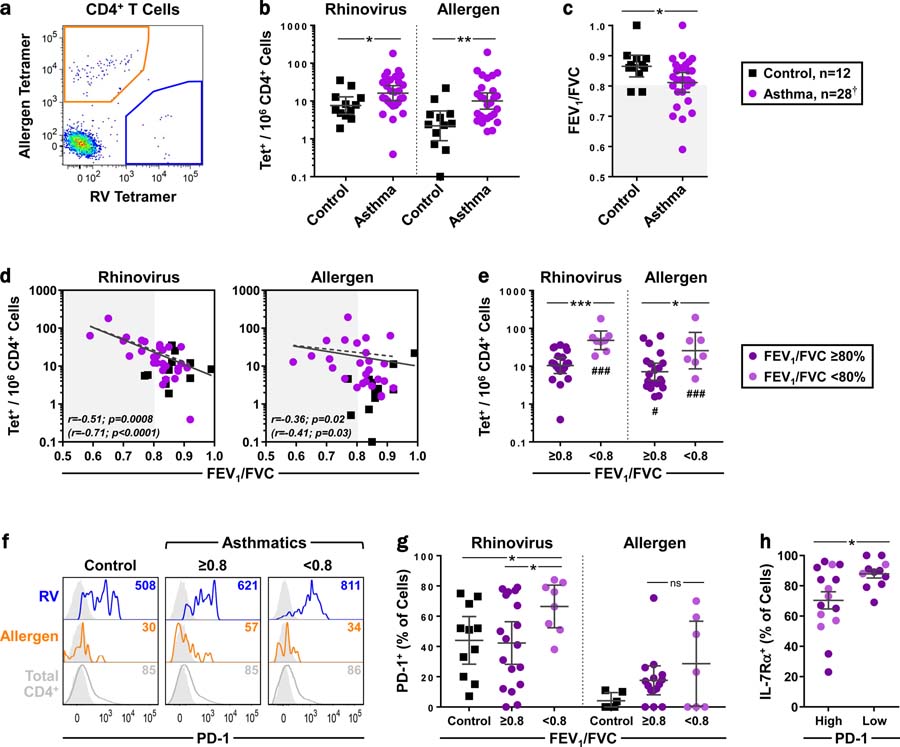
Methods: Circulating virus-specific TH1 cells and allergen-specific TH2 cells were precisely monitored before and after rhinovirus challenge in allergic asthmatic subjects (total IgE, 133-4692 IU/mL; n = 28) and healthy nonallergic controls (n = 12) using peptide/MHCII tetramers. T cells were sampled for up to 11 weeks to capture steady-state and postinfection phases. T-cell responses were analyzed in parallel with 18 cytokines in the nose, upper and lower airway symptoms, and lung function. The influence of in vivo IgE blockade was also examined.
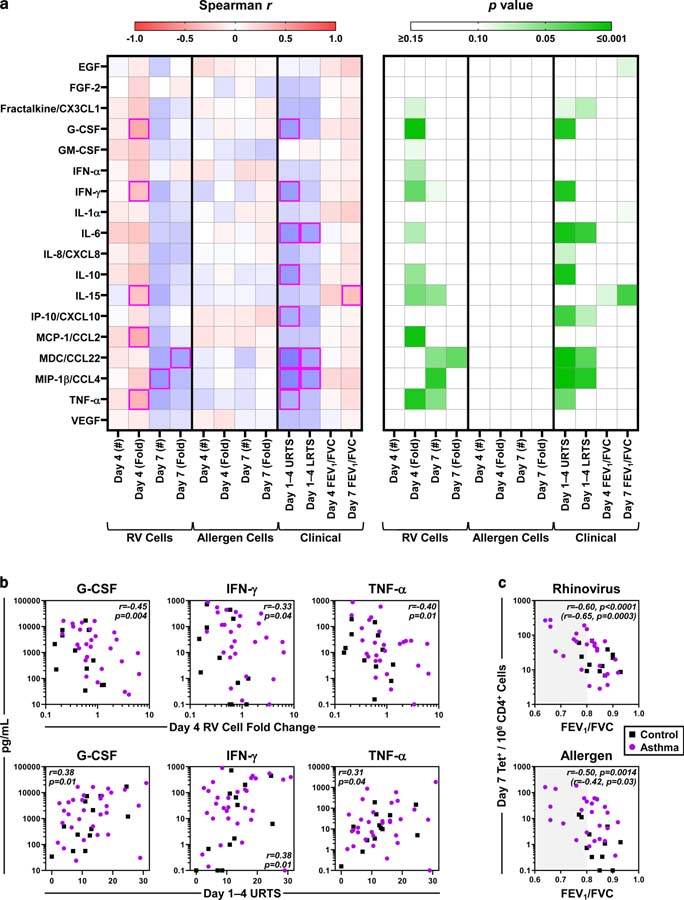
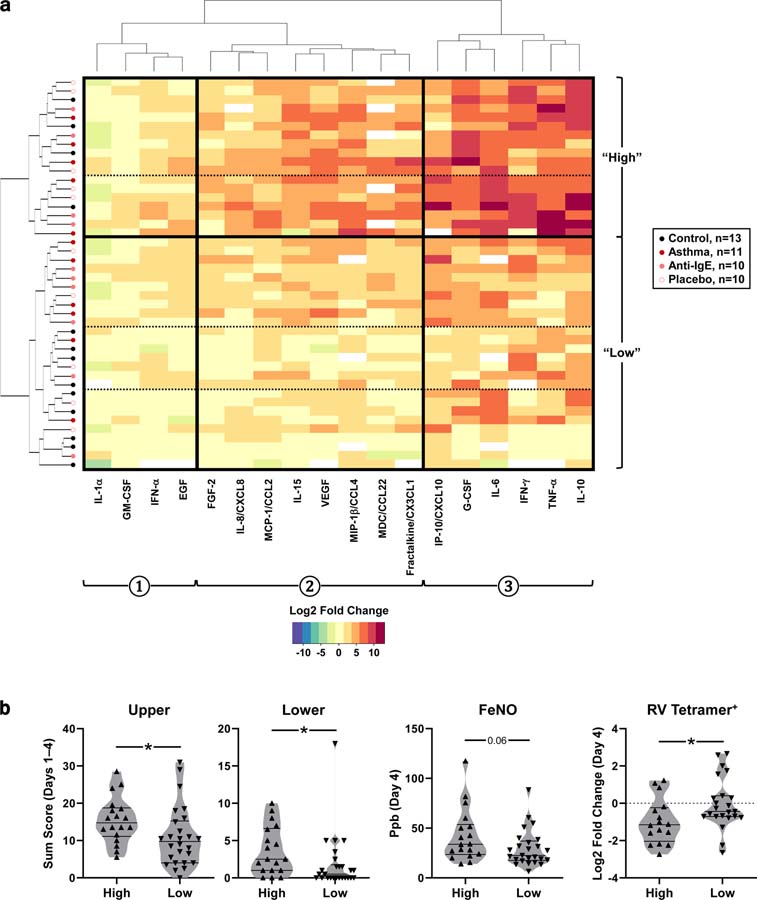
Results: In uninfected asthmatic subjects, higher numbers of circulating virus-specific PD-1+ TH1 cells, but not allergen-specific TH2 cells, were linked to worse lung function. Rhinovirus infection induced an amplified antiviral TH1 response in asthmatic subjects versus controls, with synchronized allergen-specific TH2 expansion, and production of type 1 and 2 cytokines in the nose. In contrast, TH2 responses were absent in infected asthmatic subjects who had normal lung function, and in those receiving anti-IgE. Across all subjects, early induction of a minimal set of nasal cytokines that discriminated high responders (G-CSF, IFN-γ, TNF-α) correlated with both egress of circulating virus-specific TH1 cells and worse symptoms.
Conclusions: Rhinovirus induces robust TH1 responses in allergic asthmatic subjects that may promote disease, even after the infection resolves.
Keywords: IFN; Rhinovirus; T cells; T(H)1; T(H)2; anti-IgE; asthma; cytokines; tetramers.
Copyright © 2020 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures





Comment in
-
Immune responses to rhinoviruses and asthma: Are we 3 steps closer to the door?J Allergy Clin Immunol. 2020 Sep;146(3):513-514. doi: 10.1016/j.jaci.2020.06.031. Epub 2020 Jul 14. J Allergy Clin Immunol. 2020. PMID: 32673613 No abstract available.
References
-
- Rakes GP, Arruda E, Ingram JM, Hoover GE, Zambrano JC, Hayden FG, et al. Rhinovirus and respiratory syncytial virus in wheezing children requiring emergency care IgE and eosinophil analyses. Am J Respir Crit Care Med 1999;159:785–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
