

Provider performance and facility readiness for managing infections in young infants in primary care facilities in rural Bangladesh
- PMID: 32320993
- PMCID: PMC7176463
- DOI: 10.1371/journal.pone.0229988
Provider performance and facility readiness for managing infections in young infants in primary care facilities in rural Bangladesh
Abstract
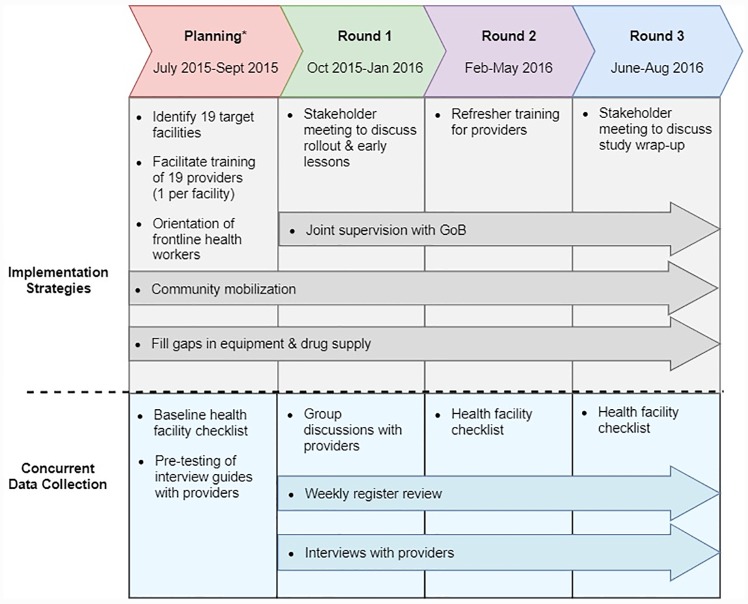
Background: Neonatal infections remain a leading cause of newborn deaths globally. In 2015, WHO issued guidelines for managing possible serious bacterial infection (PSBI) in young infants (0-59 days) using simplified antibiotic regimens when compliance with hospital referral is not feasible. Bangladesh was one of the first countries to adopt WHO's guidelines for implementation. We report results of an implementation research study that assessed facility readiness and provider performance in three rural sub-districts of Bangladesh during August 2015-August 2016.
Methods: This study took place in 19 primary health centers. Facility readiness was assessed using checklists completed by study staff at three time points. To assess provider performance, we extracted data for all infection cases from facility registers and compared providers' diagnosis and treatment against the guidelines. We plotted classification and dosage errors across the study period and superimposed a locally weighted smoothed (LOWESS) curve to analyze changes in performance over time. Focus group discussions (N = 2) and in-depth interviews (N = 28) with providers were conducted to identify barriers and facilitators for facility readiness and provider performance.
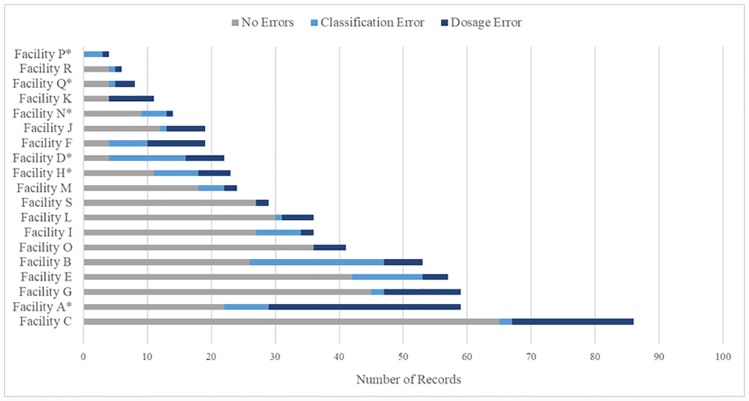
Results: At baseline, none of the facilities had adequate supply of antibiotics. During the 10-month period, 606 sick infants with signs of infection presented at the study facilities. Classification errors were identified in 14.9% (N = 90/606) of records. For infants receiving the first dose(s) of antibiotic treatment (N = 551), dosage errors were identified in 22.9% (N = 126/551) of the records. Distribution of errors varied by facility (35.7% [IQR: 24.7-57.4%]) and infection severity. Errors were highest at the beginning of the study period and decreased over time. Qualitative data suggest errors in early implementation were due to changes in providers' assessment and treatment practices, including confusion about classifying an infant with multiple signs of infection, and some providers' concerns about the efficacy of simplified antibiotic regimens.
Conclusions: Strategies to monitor early performance and targeted supports are important for enhancing implementation fidelity when introducing complex guidelines in new settings. Future research should examine providers' assessment of effectiveness of simplified treatment and address misconceptions about superiority of broader spectrum antibiotics for treating community-acquired neonatal infections in this context.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- You D, Hug L, Ejdemyr S, Beise J. Levels and trends in child mortality. Report 2015. Estimates developed by the UN Inter-agency Group for Child Mortality Estimation. 2015.
-
- Liu L, Oza S, Hogan D, Chu Y, Perin J, Zhu J, et al. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet. 2016;388(10063):3027–35. Epub 2016/11/15. 10.1016/S0140-6736(16)31593-8 . - DOI - PMC - PubMed
-
- National Institute of Population Research and Training (NIPORT) MaA, and ICF International,. Bangladesh Demographic and Health Survey 2014. Dhaka, Bangladesh, and Rockville, Maryland, USA: 2016.
-
- Baqui AH, Williams E, El-Arifeen S, Applegate JA, Mannan I, Begum N, et al. Effect of community-based newborn care on cause-specific neonatal mortality in Sylhet district, Bangladesh: findings of a cluster-randomized controlled trial. Journal of perinatology: official journal of the California Perinatal Association. 2016;36(1):71–6. 10.1038/jp.2015.139 . - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
