

Criteria for defining interictal epileptiform discharges in EEG: A clinical validation study
- PMID: 32321764
- PMCID: PMC7526669
- DOI: 10.1212/WNL.0000000000009439
Criteria for defining interictal epileptiform discharges in EEG: A clinical validation study
Abstract
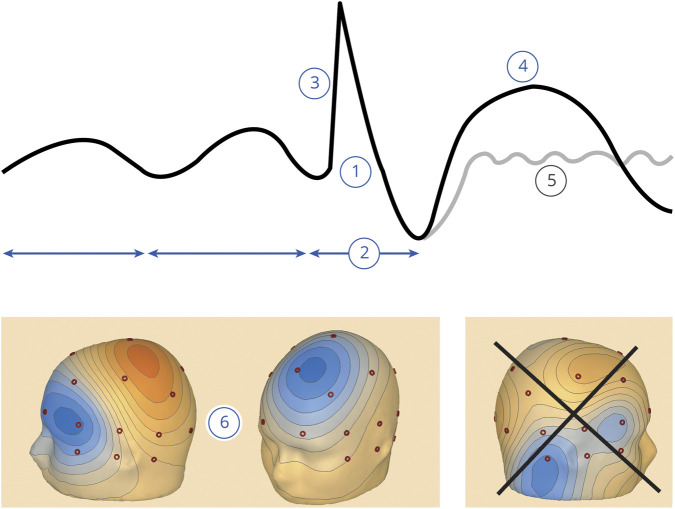
Objective: To define and validate criteria for accurate identification of EEG interictal epileptiform discharges (IEDs) using (1) the 6 sensor space criteria proposed by the International Federation of Clinical Neurophysiology (IFCN) and (2) a novel source space method. Criteria yielding high specificity are needed because EEG over-reading is a common cause of epilepsy misdiagnosis.
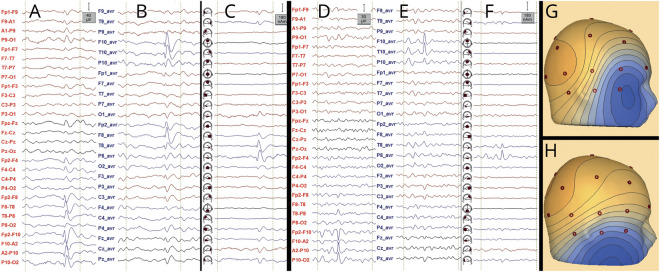
Methods: Seven raters reviewed EEG sharp transients from 100 patients with and without epilepsy (diagnosed definitively by video-EEG recording of habitual events). Raters reviewed the transients, randomized, and classified them as epileptiform or nonepileptiform in 3 separate rounds: in 2, EEG was reviewed in sensor space (scoring the presence/absence of each IFCN criterion for each transient or classifying unrestricted by criteria [expert scoring]); in the other, review and classification were performed in source space.
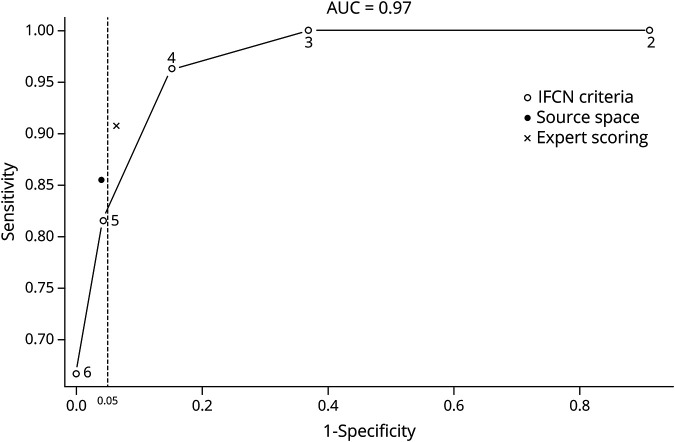
Results: Cutoff values of 4 and 5 criteria in sensor space and analysis in source space provided high accuracy (91%, 88%, and 90%, respectively), similar to expert scoring (92%). Two methods had specificity exceeding the desired threshold of 95%: using 5 IFCN criteria as cutoff and analysis in source space (both 95.65%); the sensitivity of these methods was 81.48% and 85.19%, respectively.
Conclusions: The presence of 5 IFCN criteria in sensor space and analysis in source space are optimal for clinical implementation. By extracting these objective features, diagnostic accuracy similar to expert scorings is achieved.
Classification of evidence: This study provides Class III evidence that IFCN criteria in sensor space and analysis in source space have high specificity (>95%) and sensitivity (81%-85%) for identification of IEDs.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
Comment in
-
Epileptiform discharges: Are we still defining them?Neurology. 2020 May 19;94(20):862-863. doi: 10.1212/WNL.0000000000009432. Epub 2020 Apr 22. Neurology. 2020. PMID: 32321765 No abstract available.
References
-
- Tatum WO, Rubboli G, Kaplan PW, et al. Clinical utility of EEG in diagnosing and monitoring epilepsy in adults. Clin Neurophysiol 2018;129:1056–1082. - PubMed
-
- Benbadis SR, Lin K. Errors in EEG interpretation and misdiagnosis of epilepsy. Which EEG patterns are overread? Eur Neurol 2008;59:267–271. - PubMed
-
- Pillai J, Sperling MR. Interictal EEG and the diagnosis of epilepsy. Epilepsia 2006;47(suppl 1):14–22. - PubMed
-
- Hoppe M, Wennberg R, Tai P, Pohlmann-Eden B. EEG in epilepsy; in Lozano AM, Gildenberg PL, Tasker RR, eds. Textbook of Stereotactic and Functional Neurosurgery. Berlin Heidelberg: Springer, 2009:2575–2585.
-
- Engel J Jr. A practical guide for routine EEG studies in epilepsy. J Clin Neurophysiol 1984;1:109–142. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials