

The landscape of immune cell infiltration and its clinical implications of pancreatic ductal adenocarcinoma
- PMID: 32322419
- PMCID: PMC7171261
- DOI: 10.1016/j.jare.2020.03.009
The landscape of immune cell infiltration and its clinical implications of pancreatic ductal adenocarcinoma
Abstract
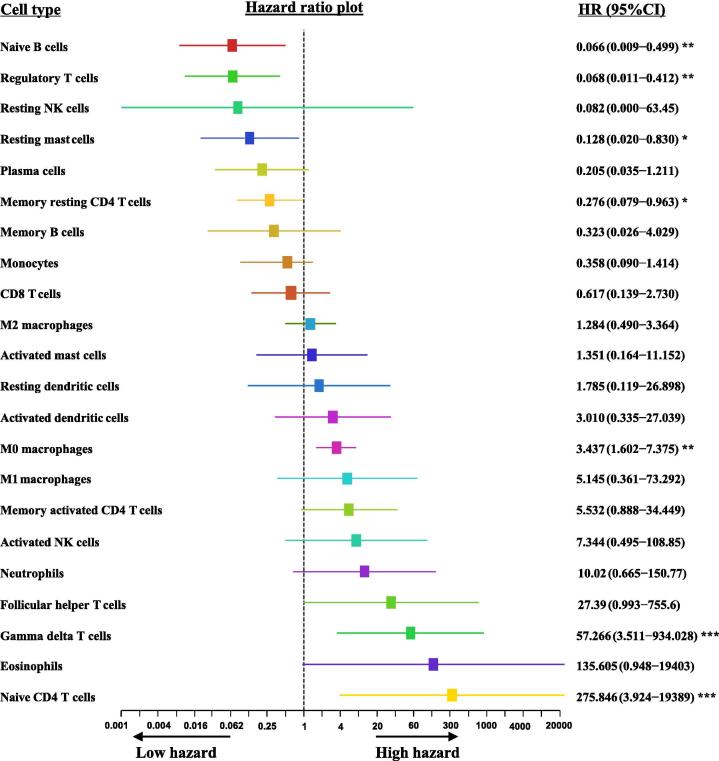
The details of the immunological microenvironment and its clinical implications for pancreatic cancer are still unclear. In this study, we obtained data from public databases, such as the Gene Expression Omnibus, the Cancer Genome Atlas Program, the International Cancer Genome Consortium Data Portal, the ArrayExpress Data Warehouse, and the cBioPortal for Cancer Genomics. We used these data to evaluate the pattern of immune cells infiltration in pancreatic ductal adenocarcinoma (PDAC) tissues. We observed that the levels of M0 macrophages and activated dendritic cells in tumor tissues were significantly higher than that in para-tumor tissues. M0 macrophages, gamma delta T cells and naive CD4 T cells were independent predictive factors of a poor outcome for PDAC patients. An immune score determined by M0 macrophages, gamma delta T cells and naive CD4 T cells could predict the survival of patients. The results of this study suggest that the infiltration of immune cells, such as M0 macrophages, may be a possible target for the treatment of PDAC. However, these findings need to be confirmed by additional studies.
Keywords: Immune cell infiltration; M0 macrophages; Pancreatic ductal adenocarcinoma; Prognosis.
© 2020 THE AUTHORS. Published by Elsevier BV on behalf of Cairo University.
Conflict of interest statement
The authors have declared no conflict of interest
Figures






References
LinkOut - more resources
Full Text Sources
Research Materials
