

Associations of Maternal Early-Pregnancy Glucose Concentrations With Placental Hemodynamics, Blood Pressure, and Gestational Hypertensive Disorders
- PMID: 32322887
- PMCID: PMC10868575
- DOI: 10.1093/ajh/hpaa070
Associations of Maternal Early-Pregnancy Glucose Concentrations With Placental Hemodynamics, Blood Pressure, and Gestational Hypertensive Disorders
Abstract
Background: Gestational diabetes mellitus is associated with increased risks of gestational hypertension and preeclampsia. We hypothesized that high maternal glucose concentrations in early pregnancy are associated with adverse placental adaptations and subsequently altered uteroplacental hemodynamics during pregnancy, predisposing to an increased risk of gestational hypertensive disorders.
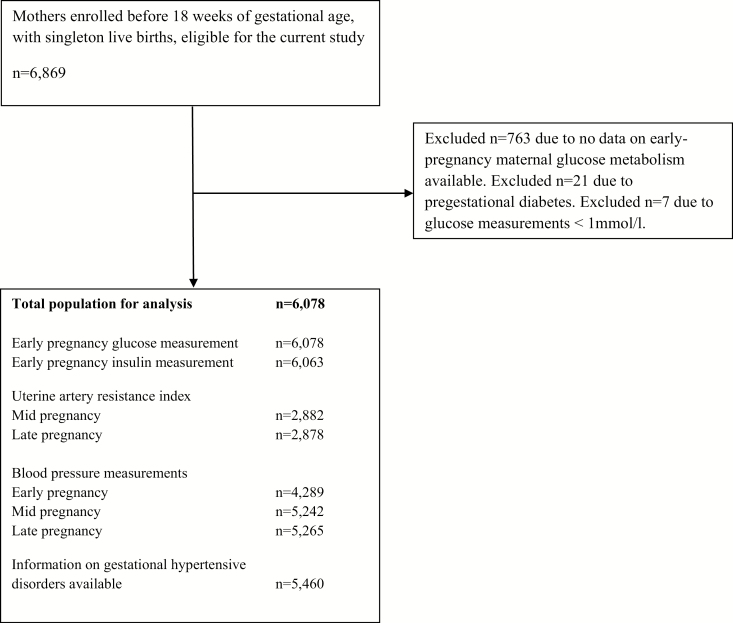
Methods: In a population-based prospective cohort study from early pregnancy onwards, among 6,078 pregnant women, maternal early-pregnancy non-fasting glucose concentrations were measured. Mid and late pregnancy uterine and umbilical artery resistance indices were assessed by Doppler ultrasound. Maternal blood pressure was measured in early, mid, and late pregnancy and the occurrence of gestational hypertensive disorders was assessed using hospital registries.
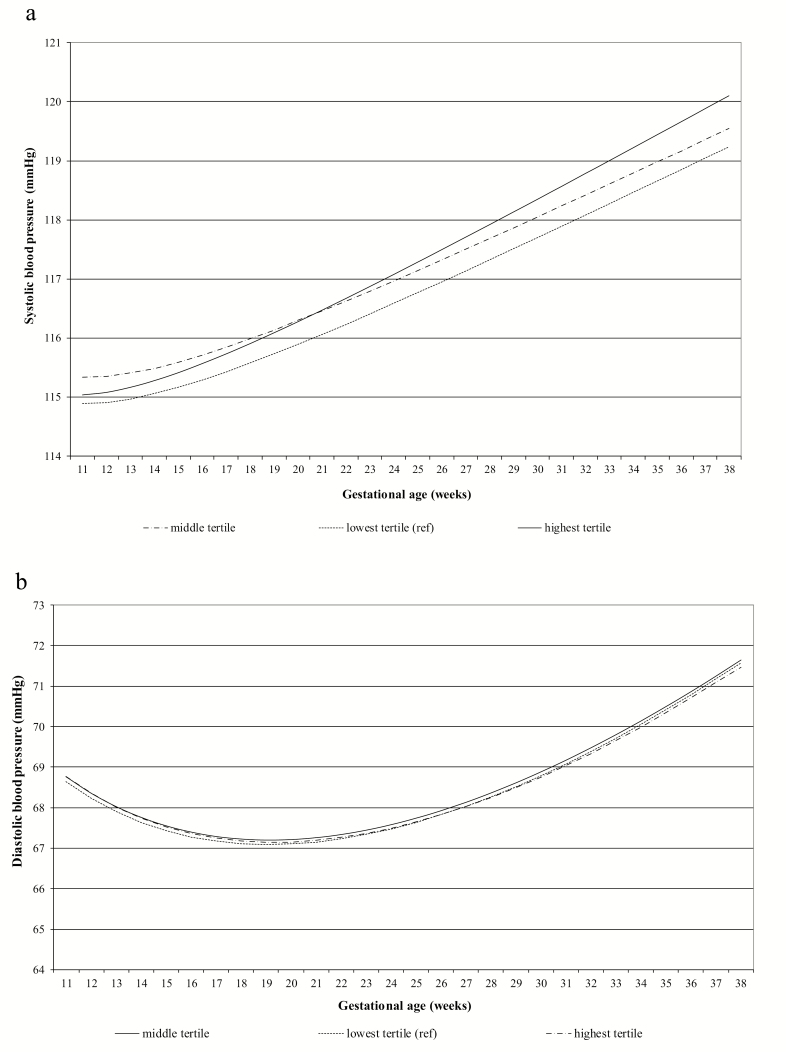
Results: Maternal early-pregnancy glucose concentrations were not associated with mid or late pregnancy placental hemodynamic markers. A 1 mmol/l increase in maternal early-pregnancy glucose concentrations was associated with 0.71 mm Hg (95% confidence interval 0.22-1.22) and 0.48 mm Hg (95% confidence interval 0.10-0.86) higher systolic and diastolic blood pressure in early pregnancy, respectively, but not with blood pressure in later pregnancy. Also, maternal glucose concentrations were not associated with the risks of gestational hypertension or preeclampsia.
Conclusions: Maternal early-pregnancy non-fasting glucose concentrations within the normal range are associated with blood pressure in early pregnancy, but do not seem to affect placental hemodynamics and the risks of gestational hypertensive disorders.
Keywords: Doppler; blood pressure; cohort; gestational hypertensive disorders; glucose; hypertension; placenta; pregnancy.
© The Author(s) 2020. Published by Oxford University Press on behalf of American Journal of Hypertension, Ltd.
Figures
References
-
- Ferrara A. Increasing prevalence of gestational diabetes mellitus: a public health perspective. Diabetes Care 2007; 30(Suppl 2):S141–S146. - PubMed
-
- Catalano PM, McIntyre HD, Cruickshank JK, McCance DR, Dyer AR, Metzger BE, Lowe LP, Trimble ER, Coustan DR, Hadden DR, Persson B, Hod M, Oats JJ; Group HSCR . The hyperglycemia and adverse pregnancy outcome study: associations of GDM and obesity with pregnancy outcomes. Diabetes Care 2012; 35:780–786. - PMC - PubMed
-
- Vega M, Mauro M, Williams Z. Direct toxicity of insulin on the human placenta and protection by metformin. Fertil Steril 2019; 111:489–496.e5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
