

Improving Molecular Therapy in the Kidney
- PMID: 32323260
- PMCID: PMC7367759
- DOI: 10.1007/s40291-020-00467-6
Improving Molecular Therapy in the Kidney
Abstract
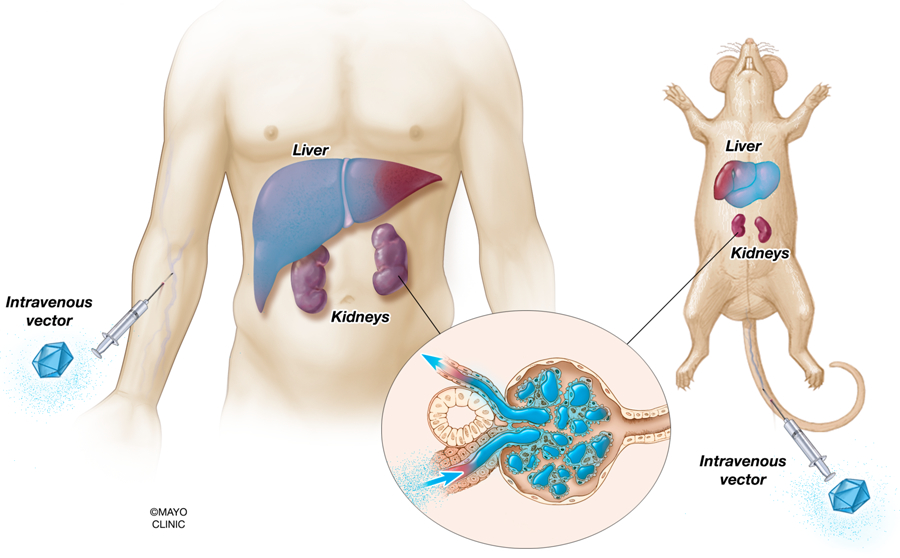
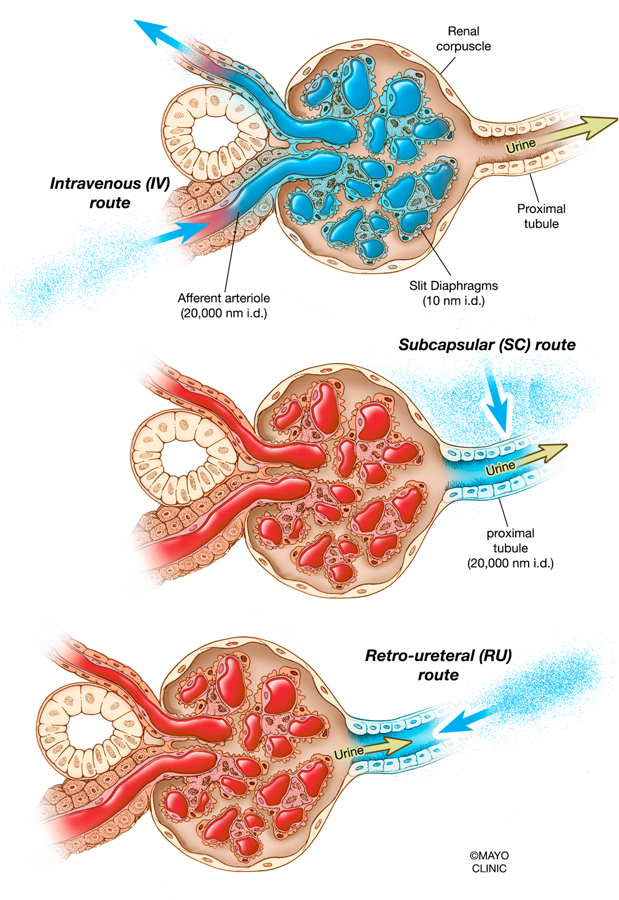
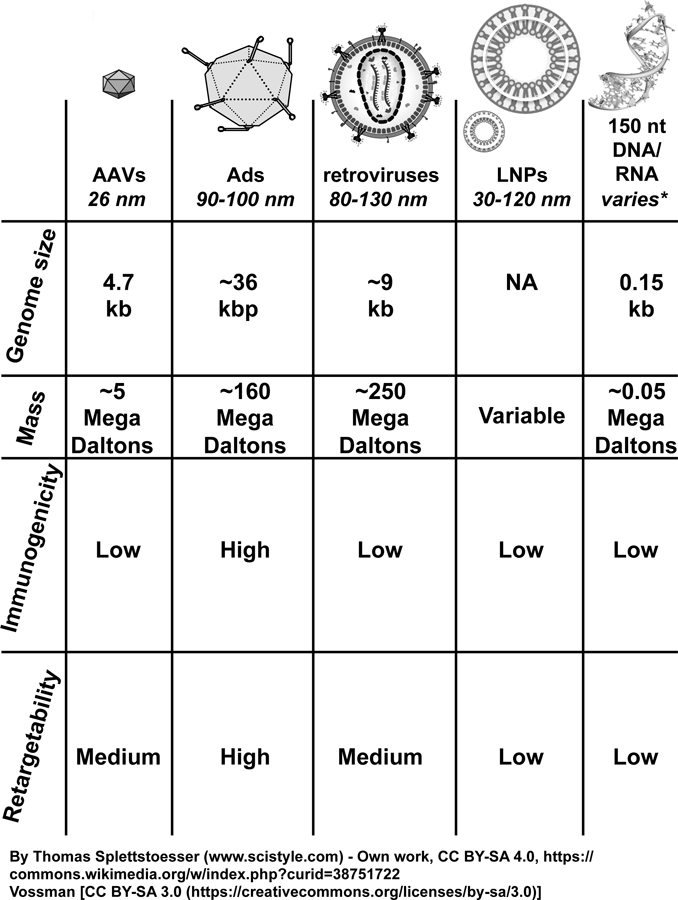
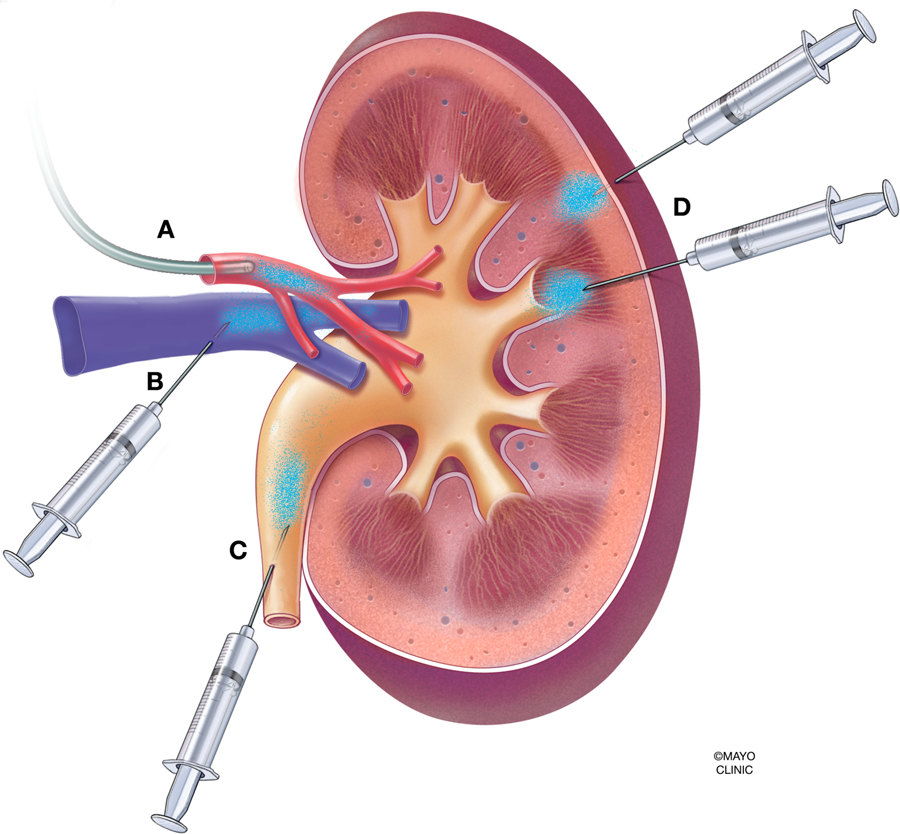
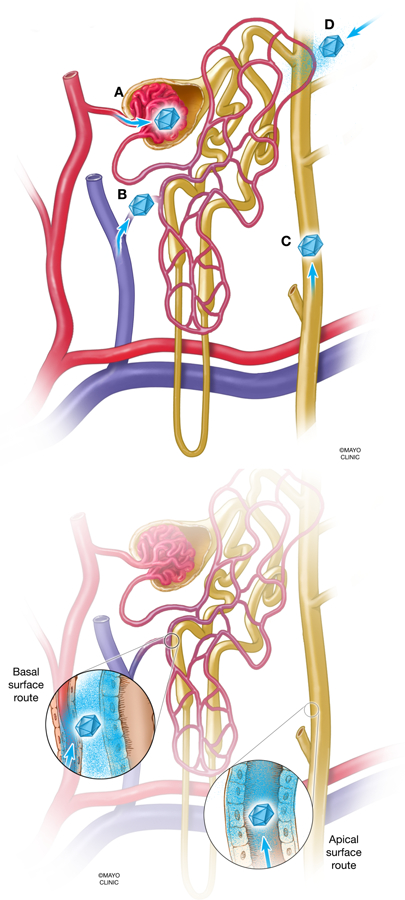
Mutations in approximately 80 genes have been implicated as the cause of various genetic kidney diseases. However, gene delivery to kidney cells from the blood is inefficient because of the natural filtering functions of the glomerulus, and research into and development of gene therapy directed toward kidney disease has lagged behind as compared with hepatic, neuromuscular, and ocular gene therapy. This lack of progress is in spite of numerous genetic mouse models of human disease available to the research community and many vectors in existence that can theoretically deliver genes to kidney cells with high efficiency. In the past decade, several groups have begun to develop novel injection techniques in mice, such as retrograde ureter, renal vein, and direct subcapsular injections to help resolve the issue of gene delivery to the kidney through the blood. In addition, the ability to retarget vectors specifically toward kidney cells has been underutilized but shows promise. This review discusses how recent advances in gene delivery to the kidney and the field of gene therapy can leverage the wealth of knowledge of kidney genetics to work toward developing gene therapy products for patients with kidney disease.
Figures
References
-
- Leung JC. Inherited renal diseases. Curr Pediatr Rev. 2014;10(2):95–100. - PubMed
-
- Boron WB, Emile. Glomerular Filtration and Renal Blood Flow Medical Physiology. 3rd ed: Elsevier; 2017. p. 739–53.e2.
-
- Murphy JJ, Myint MK, Rattner WH, Klaus R, Shallow J. The lymphatic system of the kidney. J Urol. 1958. July;80(1):1–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
