

The independent reduction in mortality associated with guideline-directed medical therapy in patients with coronary artery disease and heart failure with reduced ejection fraction
- PMID: 32324852
- PMCID: PMC8294676
- DOI: 10.1093/ehjqcco/qcaa032
The independent reduction in mortality associated with guideline-directed medical therapy in patients with coronary artery disease and heart failure with reduced ejection fraction
Abstract
Aims: Guideline-directed medical therapy (GDMT) is underutilized in patients with coronary artery disease (CAD). However, there are no studies evaluating the impact of GDMT adherence on mortality among patients with CAD and heart failure with reduced ejection fraction (HFrEF). We sought to investigate the association of GDMT adherence with long-term mortality in patients with CAD and HFrEF.
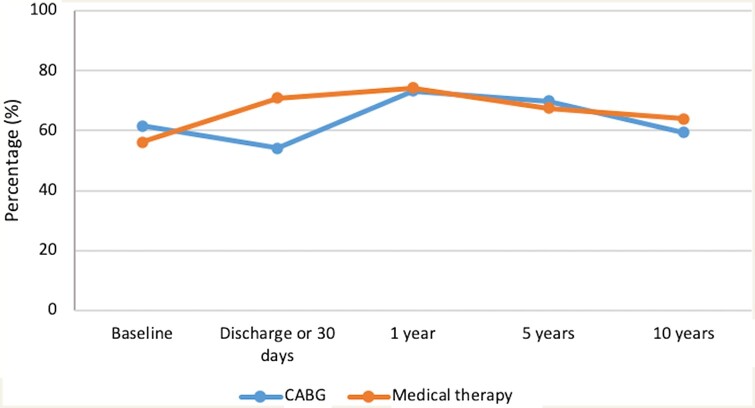
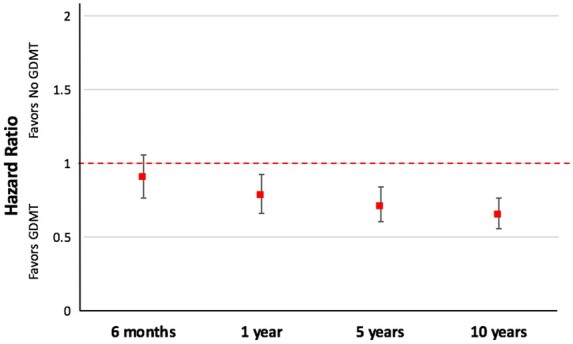
Methods and results: Surgical Treatment for Ischaemic Heart Failure (STICH) was a trial of patients with an left ventricular ejection fraction ≤35% and CAD amenable to coronary artery bypass graft surgery (CABG) who were randomized to CABG plus medical therapy (N = 610) or medical therapy alone (N = 602). Median follow-up time was 9.8 years. We defined GDMT for the treatment of CAD and HFrEF as the combination of at least one antiplatelet drug, a statin, a beta-blocker, and an angiotensin-converting enzyme inhibitor or angiotensin receptor blocker. The primary outcome was all-cause mortality. Assessment of the independent association between GDMT and mortality was performed using multivariable Cox regression with GDMT as a time-dependent covariate. In the CABG arm, 63.6% of patients were on GDMT throughout the study period compared to 66.5% of patients in the medical therapy arm (P = 0.3). GDMT was independently associated with a significant reduction in mortality (hazard ratio 0.65, 95% confidence interval 0.56-0.76; P < 0.001).
Conclusion: GDMT is associated with reduced mortality in patients with CAD and HFrEF independent of revascularization with CABG. Strategies to improve GDMT adherence in this population are needed to maximize survival.
Keywords: Cardiomyopathy; Coronary artery disease; Heart failure; Outcome.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS. et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Rev Esp Cardiol (Engl Ed) 2016;69:1167. - PubMed
-
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, Prescott E, Storey RF, Deaton C, Cuisset T, Agewall S, Dickstein K, Edvardsen T, Escaned J, Gersh BJ, Svitil P, Gilard M, Hasdai D, Hatala R, Mahfoud F, Masip J, Muneretto C, Valgimigli M, Achenbach S, Bax JJ; ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J 2020;41:407–477. - PubMed
-
- Hiratzka LF, Eagle KA, Liang L, Fonarow GC, LaBresh KA, Peterson ED; Get with the Guidelines Steering Committee. Atherosclerosis secondary prevention performance measures after coronary bypass graft surgery compared with percutaneous catheter intervention and nonintervention patients in the Get With the Guidelines database. Circulation 2007;116:I207–I212. - PubMed
-
- Newby LK, Allen LaPointe NM, Chen AY, Kramer JM, Hammill BG, DeLong ER. et al. Long-term adherence to evidence-based secondary prevention therapies in coronary artery disease. Circulation 2006;113:203–212. - PubMed
-
- Borden WV, Redbery RF, Mushlin AI, Dai D, Kaltenbach LA, Spertus JA.. Patterns and intensity of medical therapy in patients undergoing percutaneous coronary intervention. JAMA 2011;305:1882–1889. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
