

Early Inspiratory Effort Assessment by Esophageal Manometry Predicts Noninvasive Ventilation Outcome in De Novo Respiratory Failure. A Pilot Study
- PMID: 32325004
- PMCID: PMC7427381
- DOI: 10.1164/rccm.201912-2512OC
Early Inspiratory Effort Assessment by Esophageal Manometry Predicts Noninvasive Ventilation Outcome in De Novo Respiratory Failure. A Pilot Study
Abstract
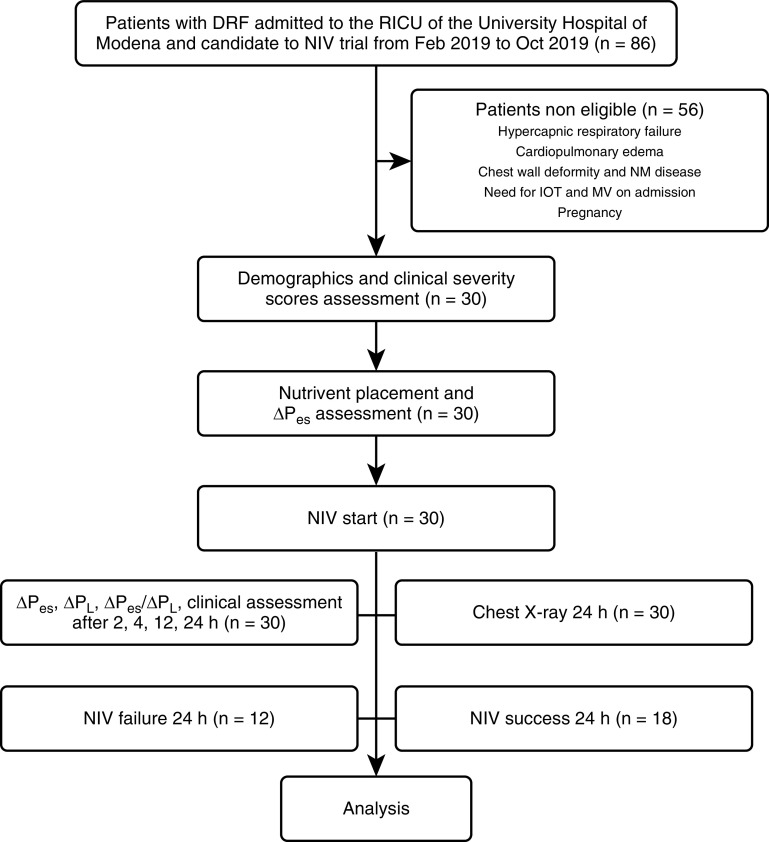
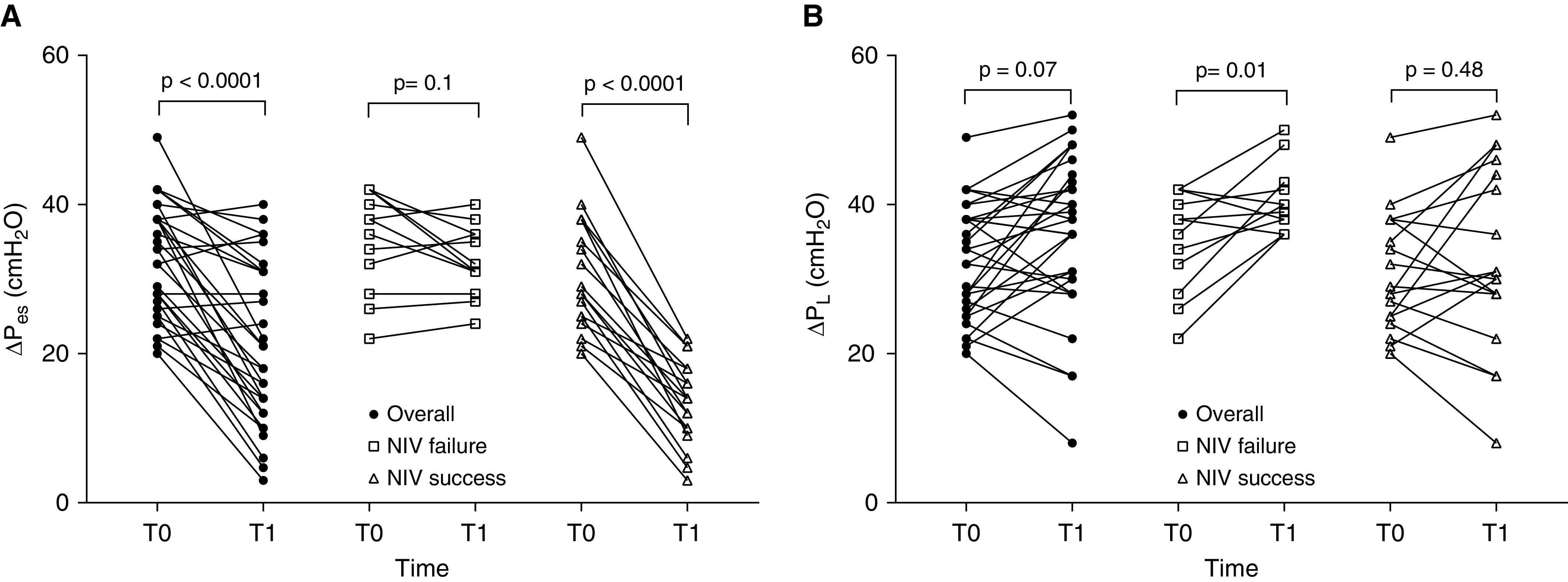
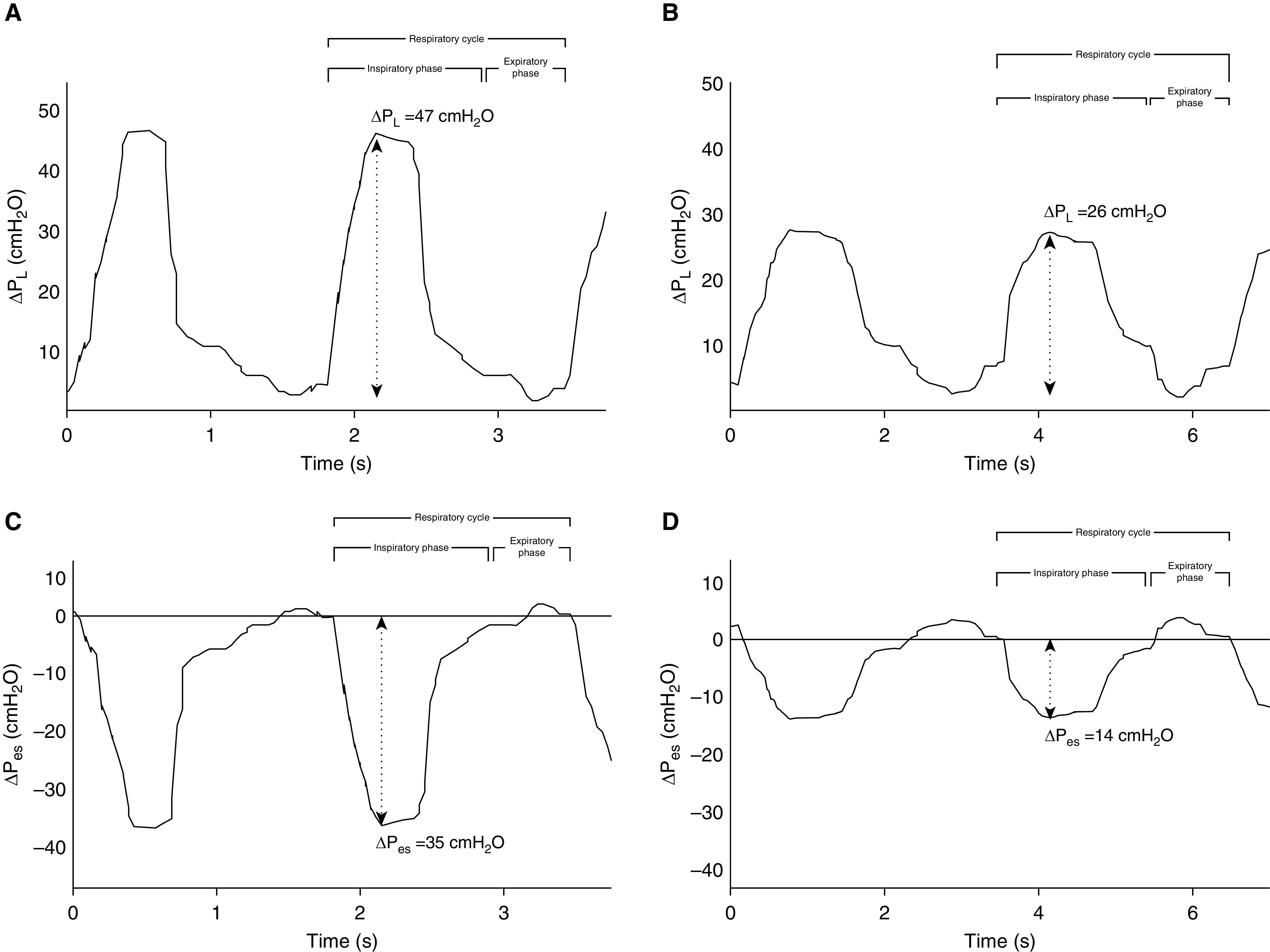
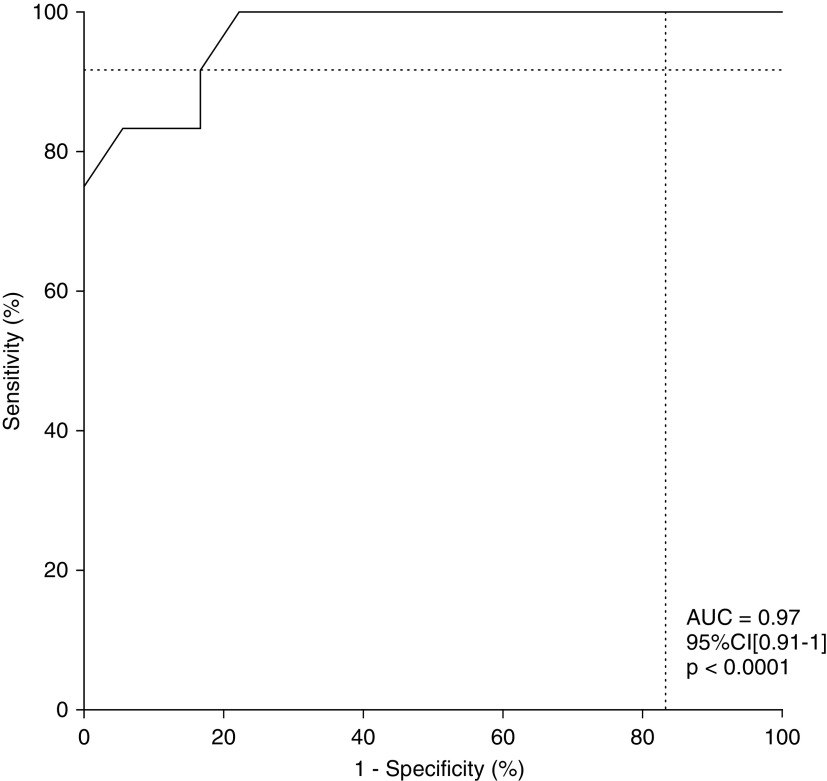
Rationale: The role of inspiratory effort still has to be determined as a potential predictor of noninvasive mechanical ventilation (NIV) failure in acute hypoxic de novo respiratory failure.Objectives: To explore the hypothesis that inspiratory effort might be a major determinant of NIV failure in these patients.Methods: Thirty consecutive patients with acute hypoxic de novo respiratory failure admitted to a single center and candidates for a 24-hour NIV trial were enrolled. Clinical features, tidal change in esophageal pressure (ΔPes), tidal change in dynamic transpulmonary pressure (ΔPl), expiratory Vt, and respiratory rate were recorded on admission and 2-4 to 12-24 hours after NIV start and were tested for correlation with outcomes.Measurements and Main Results: ΔPes and ΔPes/ΔPl ratio were significantly lower 2 hours after NIV start in patients who successfully completed the NIV trial (n = 18) compared with those who needed endotracheal intubation (n = 12) (median [interquartile range], 11 [8-15] cm H2O vs. 31.5 [30-36] cm H2O; P < 0.0001), whereas other variables differed later. ΔPes was not related to other predictors of NIV failure at baseline. NIV-induced reduction in ΔPes of 10 cm H2O or more after 2 hours of treatment was strongly associated with avoidance of intubation and represented the most accurate predictor of treatment success (odds ratio, 15; 95% confidence interval, 2.8-110; P = 0.001 and area under the curve, 0.97; 95% confidence interval, 0.91-1; P < 0.0001).Conclusions: The magnitude of inspiratory effort relief as assessed by ΔPes variation within the first 2 hours of NIV was an early and accurate predictor of NIV outcome at 24 hours.Clinical trial registered with www.clinicaltrials.gov (NCT03826797).
Keywords: acute respiratory distress syndrome; esophageal pressure swings; noninvasive mechanical ventilation; respiratory failure; transpulmonary pressure.
Figures
Comment in
-
The Dark Side of Spontaneous Breathing during Noninvasive Ventilation. From Hypothesis to Theory.Am J Respir Crit Care Med. 2020 Aug 15;202(4):482-484. doi: 10.1164/rccm.202005-1612ED. Am J Respir Crit Care Med. 2020. PMID: 32432934 Free PMC article. No abstract available.
-
Should We Monitor Pulsus Paradoxus via Pulse Oximetry in Patients with COVID-19 and Acute Respiratory Failure?Am J Respir Crit Care Med. 2020 Sep 1;202(5):770-771. doi: 10.1164/rccm.202004-1504LE. Am J Respir Crit Care Med. 2020. PMID: 32492351 Free PMC article. No abstract available.
-
Reply to Tuffet et al. and to Michard and Shelley.Am J Respir Crit Care Med. 2020 Sep 1;202(5):771-772. doi: 10.1164/rccm.202005-1730LE. Am J Respir Crit Care Med. 2020. PMID: 32492359 Free PMC article. No abstract available.
-
Continued Vigorous Inspiratory Effort as a Predictor of Noninvasive Ventilation Failure.Am J Respir Crit Care Med. 2020 Dec 15;202(12):1738-1739. doi: 10.1164/rccm.202008-3217LE. Am J Respir Crit Care Med. 2020. PMID: 32945690 Free PMC article. No abstract available.
-
Reply to Spinelli et al. and to Jha: Continued Vigorous Inspiratory Effort as a Predictor of Noninvasive Ventilation Failure.Am J Respir Crit Care Med. 2020 Dec 15;202(12):1739-1741. doi: 10.1164/rccm.202008-3049LE. Am J Respir Crit Care Med. 2020. PMID: 32945694 Free PMC article. No abstract available.
References
-
- Putensen C, Mutz NJ, Putensen-Himmer G, Zinserling J. Spontaneous breathing during ventilatory support improves ventilation-perfusion distributions in patients with acute respiratory distress syndrome. Am J Respir Crit Care Med. 1999;159:1241–1248. - PubMed
-
- Girard TD, Kress JP, Fuchs BD, Thomason JW, Schweickert WD, Pun BT, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (awakening and breathing controlled trial): a randomised controlled trial. Lancet. 2008;371:126–134. - PubMed
-
- Yoshida T, Fujino Y, Amato MB, Kavanagh BP. Fifty years of research in ARDS. Spontaneous breathing during mechanical ventilation. Risks, mechanisms, and management. Am J Respir Crit Care Med. 2017;195:985–992. - PubMed
-
- Bellani G, Laffey JG, Pham T, Madotto F, Fan E, Brochard L, et al. LUNG SAFE Investigators; ESICM Trials Group. Noninvasive ventilation of patients with acute respiratory distress syndrome. Insights from the LUNG SAFE study. Am J Respir Crit Care Med. 2017;195:67–77. - PubMed
-
- Demoule A, Girou E, Richard JC, Taille S, Brochard L. Benefits and risks of success or failure of noninvasive ventilation. Intensive Care Med. 2006;32:1756–1765. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
