

Assessing the Accuracy of a Deep Learning Method to Risk Stratify Indeterminate Pulmonary Nodules
- PMID: 32326730
- PMCID: PMC7365375
- DOI: 10.1164/rccm.201903-0505OC
Assessing the Accuracy of a Deep Learning Method to Risk Stratify Indeterminate Pulmonary Nodules
Abstract
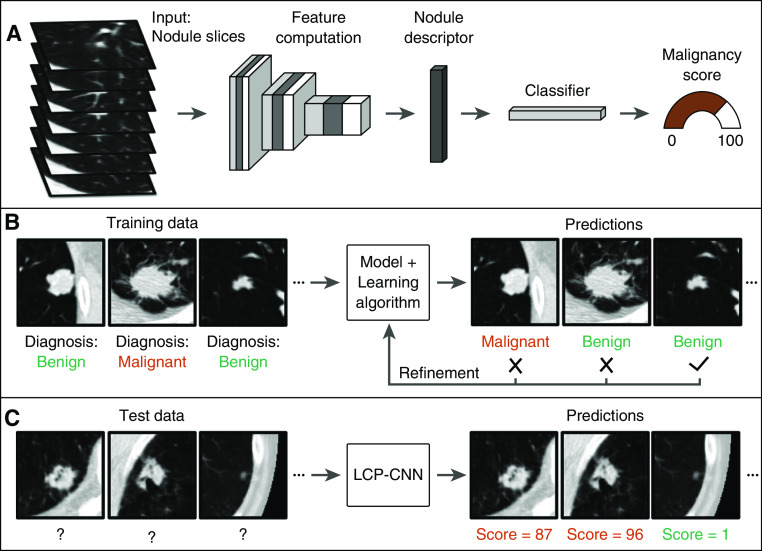
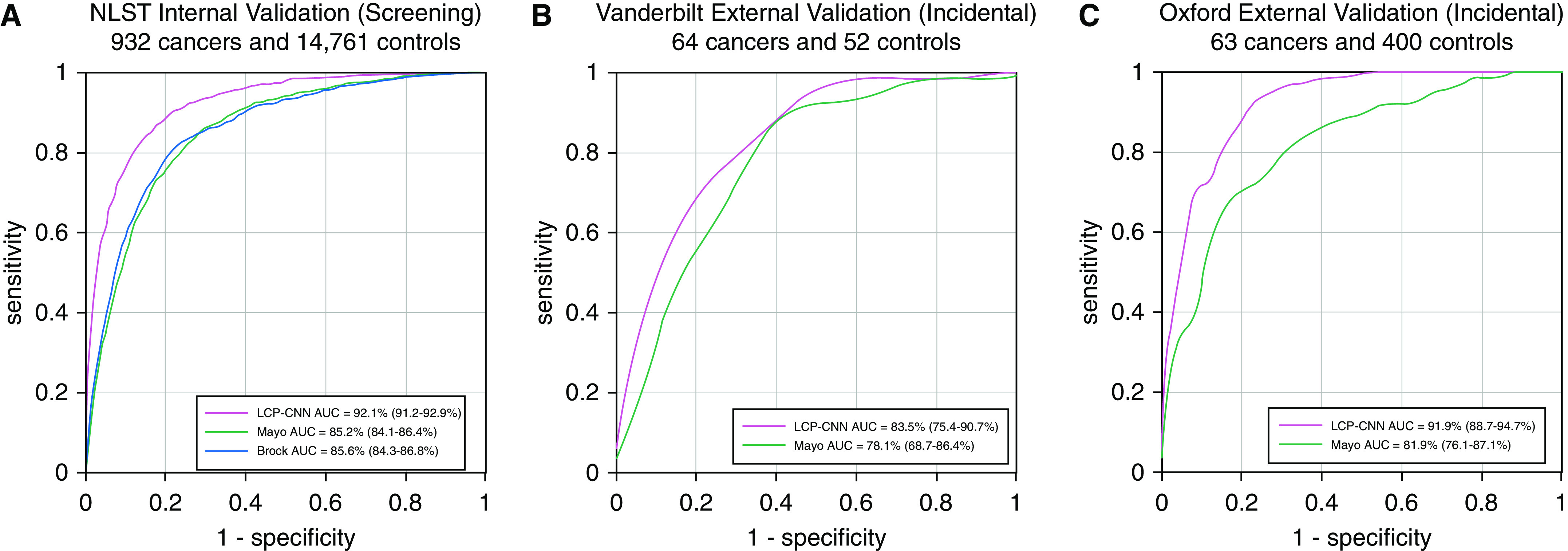
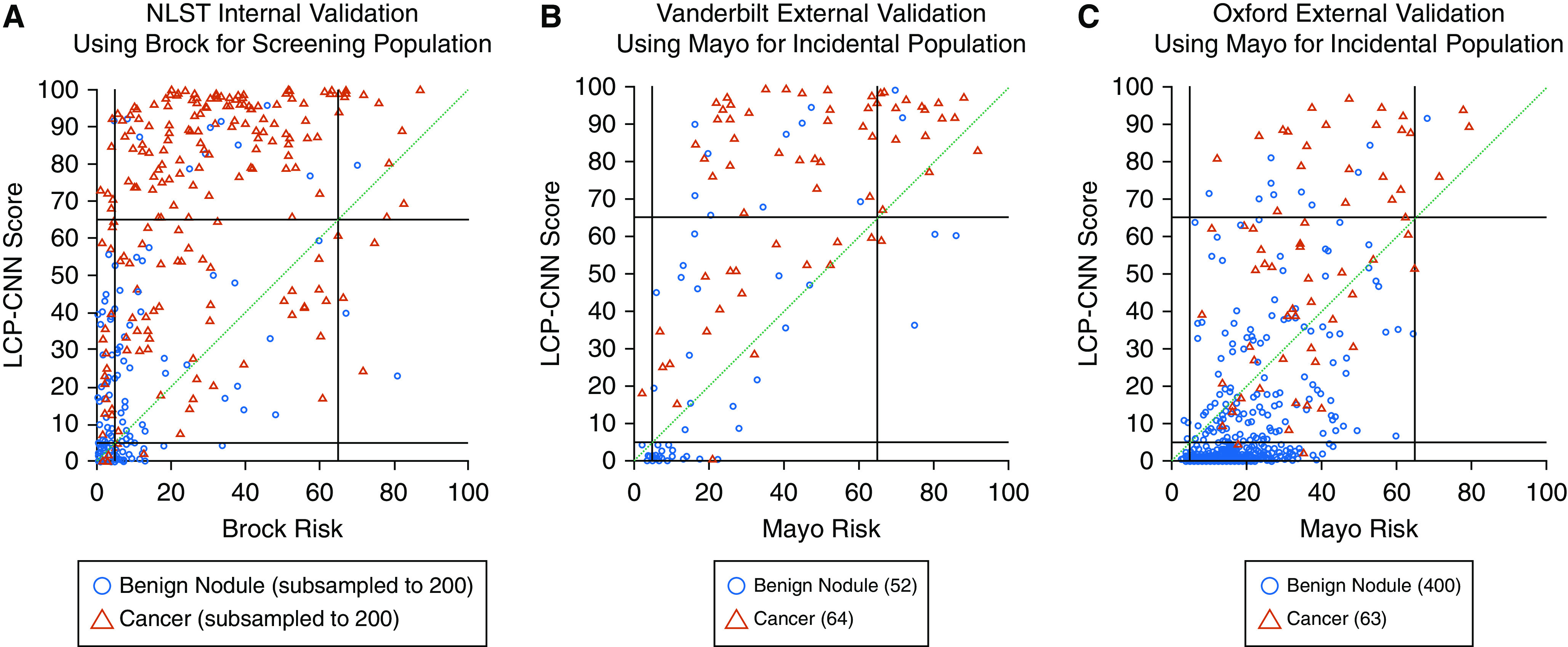
Rationale: The management of indeterminate pulmonary nodules (IPNs) remains challenging, resulting in invasive procedures and delays in diagnosis and treatment. Strategies to decrease the rate of unnecessary invasive procedures and optimize surveillance regimens are needed.Objectives: To develop and validate a deep learning method to improve the management of IPNs.Methods: A Lung Cancer Prediction Convolutional Neural Network model was trained using computed tomography images of IPNs from the National Lung Screening Trial, internally validated, and externally tested on cohorts from two academic institutions.Measurements and Main Results: The areas under the receiver operating characteristic curve in the external validation cohorts were 83.5% (95% confidence interval [CI], 75.4-90.7%) and 91.9% (95% CI, 88.7-94.7%), compared with 78.1% (95% CI, 68.7-86.4%) and 81.9 (95% CI, 76.1-87.1%), respectively, for a commonly used clinical risk model for incidental nodules. Using 5% and 65% malignancy thresholds defining low- and high-risk categories, the overall net reclassifications in the validation cohorts for cancers and benign nodules compared with the Mayo model were 0.34 (Vanderbilt) and 0.30 (Oxford) as a rule-in test, and 0.33 (Vanderbilt) and 0.58 (Oxford) as a rule-out test. Compared with traditional risk prediction models, the Lung Cancer Prediction Convolutional Neural Network was associated with improved accuracy in predicting the likelihood of disease at each threshold of management and in our external validation cohorts.Conclusions: This study demonstrates that this deep learning algorithm can correctly reclassify IPNs into low- or high-risk categories in more than a third of cancers and benign nodules when compared with conventional risk models, potentially reducing the number of unnecessary invasive procedures and delays in diagnosis.
Keywords: computer-aided image analysis; early detection; lung cancer; neural networks; risk stratification.
Figures
Comment in
-
Radiomics-based Management of Indeterminate Lung Nodules? Are We There Yet?Am J Respir Crit Care Med. 2020 Jul 15;202(2):165-167. doi: 10.1164/rccm.202004-1279ED. Am J Respir Crit Care Med. 2020. PMID: 32383972 Free PMC article. No abstract available.
-
Reply to Wilson: Risk-Stratifying Pulmonary Nodules.Am J Respir Crit Care Med. 2021 Jan 1;203(1):150. doi: 10.1164/rccm.202008-3370LE. Am J Respir Crit Care Med. 2021. PMID: 33141593 Free PMC article. No abstract available.
-
Risk-Stratifying Pulmonary Nodules.Am J Respir Crit Care Med. 2021 Jan 1;203(1):149-150. doi: 10.1164/rccm.202008-3057LE. Am J Respir Crit Care Med. 2021. PMID: 33141600 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J Clin. 2020;70:7–30. - PubMed
-
- American Lung Association. State of lung cancer. 2019. [accessed 2019 Feb 1]. Available from: https://www.lung.org/research/state-of-lung-cancer.
-
- American Cancer Society. Cancer facts & figures. 2018. [accessed 2019 Feb 1]. Available from: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-....
-
- De Koning HJ.NELSON study shows CT screening for nodule volume management reduces lung cancer mortality by 26 percent in men. Presented at the IASLC 19th World Conference on Lung Cancer. Sept 23–26, 2018; Toronto, Canada
