

Hepatitis C prevalence and risk factors in Georgia, 2015: setting a baseline for elimination
- PMID: 32326913
- PMCID: PMC6696670
- DOI: 10.1186/s12889-019-6784-3
Hepatitis C prevalence and risk factors in Georgia, 2015: setting a baseline for elimination
Abstract
Background: The country of Georgia launched the world's first Hepatitis C Virus (HCV) Elimination Program in 2015 and set a 90% prevalence reduction goal for 2020. We conducted a nationally representative HCV seroprevalence survey to establish baseline prevalence to measure progress toward elimination over time.
Methods: A cross-sectional seroprevalence survey was conducted in 2015 among adults aged ≥18 years using a stratified, multi-stage cluster design (n = 7000). Questionnaire variables included demographic, medical, and behavioral risk characteristics and HCV-related knowledge. Blood specimens were tested for antibodies to HCV (anti-HCV) and HCV RNA. Frequencies were computed for HCV prevalence, risk factors, and HCV-related knowledge. Associations between anti-HCV status and potential risk factors were calculated using logistic regression.
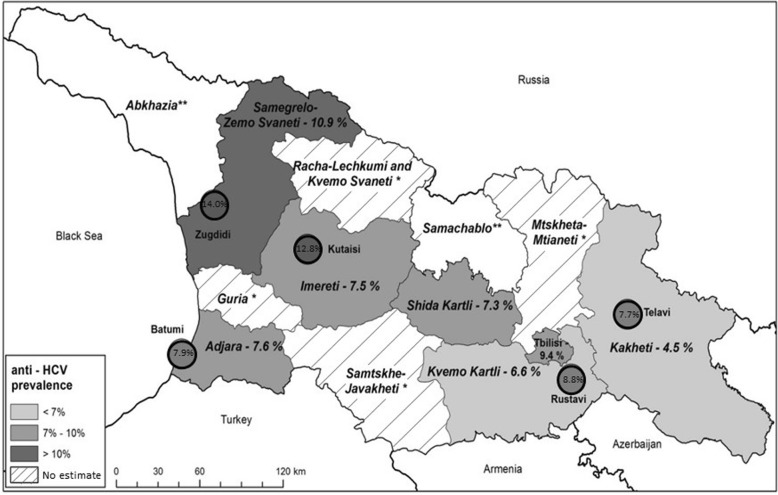
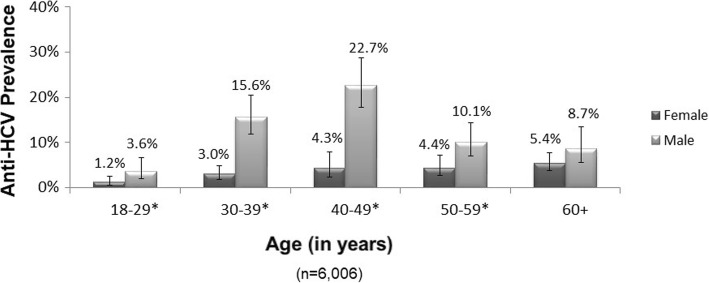
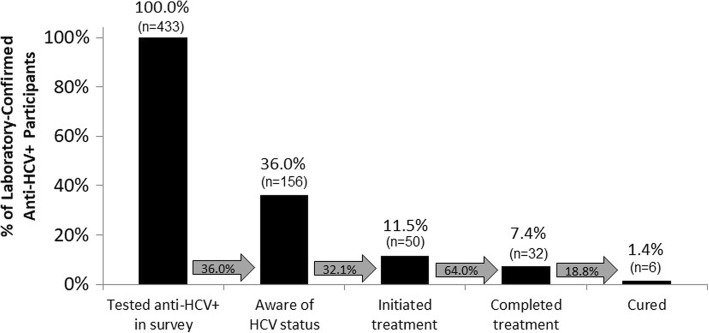
Results: National anti-HCV seroprevalence in Georgia was 7.7% (95% confidence interval (CI) = 6.7, 8.9); HCV RNA prevalence was 5.4% (95% CI = 4.6, 6.4). Testing anti-HCV+ was significantly associated with male sex, unemployment, urban residence, history of injection drug use (IDU), incarceration, blood transfusion, tattoos, frequent dental cleanings, medical injections, dialysis, and multiple lifetime sexual partners. History of IDU (adjusted odds ratio (AOR) = 21.4, 95% CI = 12.3, 37.4) and blood transfusion (AOR = 4.5, 95% CI = 2.8, 7.2) were independently, significantly associated with testing anti-HCV+ after controlling for sex, age, urban vs. rural residence, and history of incarceration. Among anti-HCV+ participants, 64.0% were unaware of their HCV status, and 46.7% did not report IDU or blood transfusion as a risk factor.
Conclusions: Georgia has a high HCV burden, and a majority of infected persons are unaware of their status. Ensuring a safe blood supply, implementing innovative screening strategies beyond a risk-based approach, and intensifying prevention efforts among persons who inject drugs are necessary steps to reach Georgia's HCV elimination goal.
Keywords: Georgia; Global health security; HCV; HCV elimination; HCV prevention; Hepatitis C virus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- World Health Organization. Global Hepatitis Report 2017 [Available from: http://apps.who.int/iris/bitstream/10665/255016/1/9789241565455-eng.pdf?.... Accessed 19 Jul 2017.]
-
- Institute of Medicine. Hepatitis and liver cancer: a National Strategy for prevention and control of hepatitis B and C. Washington, DC; 2010. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
