

The clinical relevance of oliguria in the critically ill patient: analysis of a large observational database
- PMID: 32326981
- PMCID: PMC7181534
- DOI: 10.1186/s13054-020-02858-x
The clinical relevance of oliguria in the critically ill patient: analysis of a large observational database
Abstract
Background: Urine output is widely used as one of the criteria for the diagnosis and staging of acute renal failure, but few studies have specifically assessed the role of oliguria as a marker of acute renal failure or outcomes in general intensive care unit (ICU) patients. Using a large multinational database, we therefore evaluated the occurrence of oliguria (defined as a urine output < 0.5 ml/kg/h) in acutely ill patients and its association with the need for renal replacement therapy (RRT) and outcome.
Methods: International observational study. All adult (> 16 years) patients in the ICON audit who had a urine output measurement on the day of admission were included. To investigate the association between oliguria and mortality, we used a multilevel analysis.
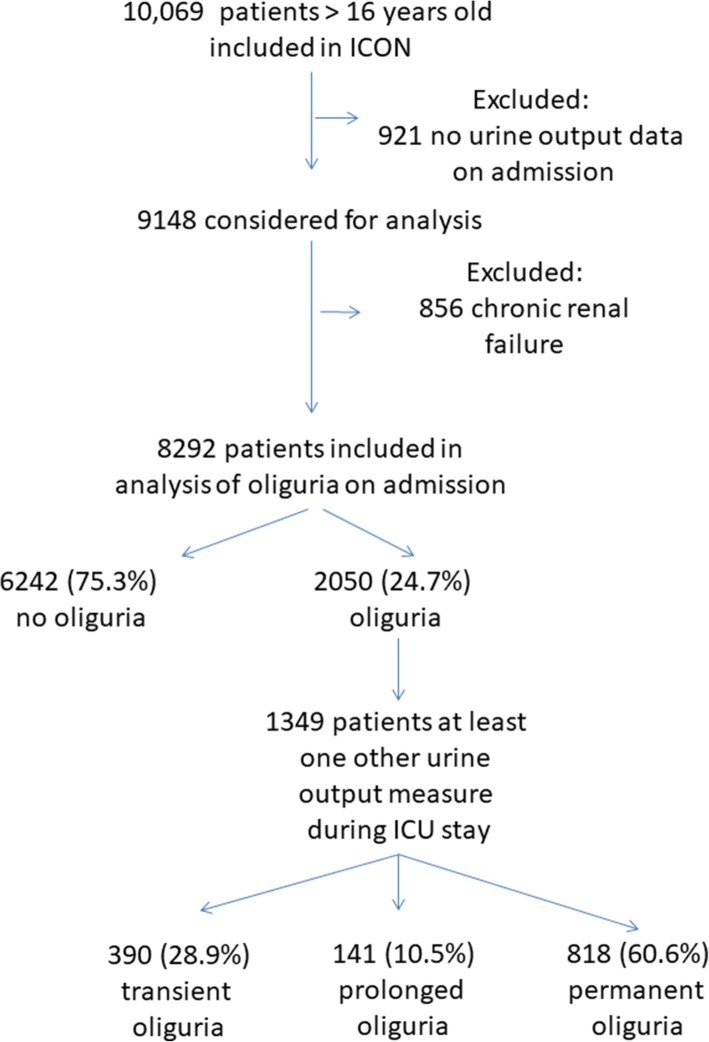
Results: Of the 8292 patients included, 2050 (24.7%) were oliguric during the first 24 h of admission. Patients with oliguria on admission who had at least one additional 24-h urine output recorded during their ICU stay (n = 1349) were divided into three groups: transient-oliguria resolved within 48 h after the admission day (n = 390 [28.9%]), prolonged-oliguria resolved > 48 h after the admission day (n = 141 [10.5%]), and permanent-oliguria persisting for the whole ICU stay or again present at the end of the ICU stay (n = 818 [60.6%]). ICU and hospital mortality rates were higher in patients with oliguria than in those without, except for patients with transient oliguria who had significantly lower mortality rates than non-oliguric patients. In multilevel analysis, the need for RRT was associated with a significantly higher risk of death (OR = 1.51 [95% CI 1.19-1.91], p = 0.001), but the presence of oliguria on admission was not (OR = 1.14 [95% CI 0.97-1.34], p = 0.103).
Conclusions: Oliguria is common in ICU patients and may have a relatively benign nature if only transient. The duration of oliguria and need for RRT are associated with worse outcome.
Keywords: Mortality; Renal replacement therapy; Urine output.
Conflict of interest statement
Marc Leone reports receiving consulting fees from Amomed and Aguettant; lecture fees from MSD, Pfizer, Octapharma, 3 M, Aspen, Orion; travel support from LFB; and grant support from PHRC IR and his institution.
JLV is the Editor-in-Chief of
The other authors declare that they have no relevant financial interests.
Figures
References
-
- Kidney Disease Outcomes Quality Initiative KDIGO clinical practice guidelines for acute kidney injury. Kidney Int Suppl. 2012;2:1–138. doi: 10.1038/kisup.2012.1. - DOI
-
- Vincent JL, Moreno R, Takala J, Willatts S, de Mendonca A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–710. doi: 10.1007/BF01709751. - DOI - PubMed
