

Diabetic Agents, From Metformin to SGLT2 Inhibitors and GLP1 Receptor Agonists: JACC Focus Seminar
- PMID: 32327107
- PMCID: PMC7219531
- DOI: 10.1016/j.jacc.2020.02.056
Diabetic Agents, From Metformin to SGLT2 Inhibitors and GLP1 Receptor Agonists: JACC Focus Seminar
Erratum in
-
Correction.J Am Coll Cardiol. 2020 Oct 6;76(14):1719-1722. doi: 10.1016/j.jacc.2020.08.023. J Am Coll Cardiol. 2020. PMID: 33004141 No abstract available.
Abstract
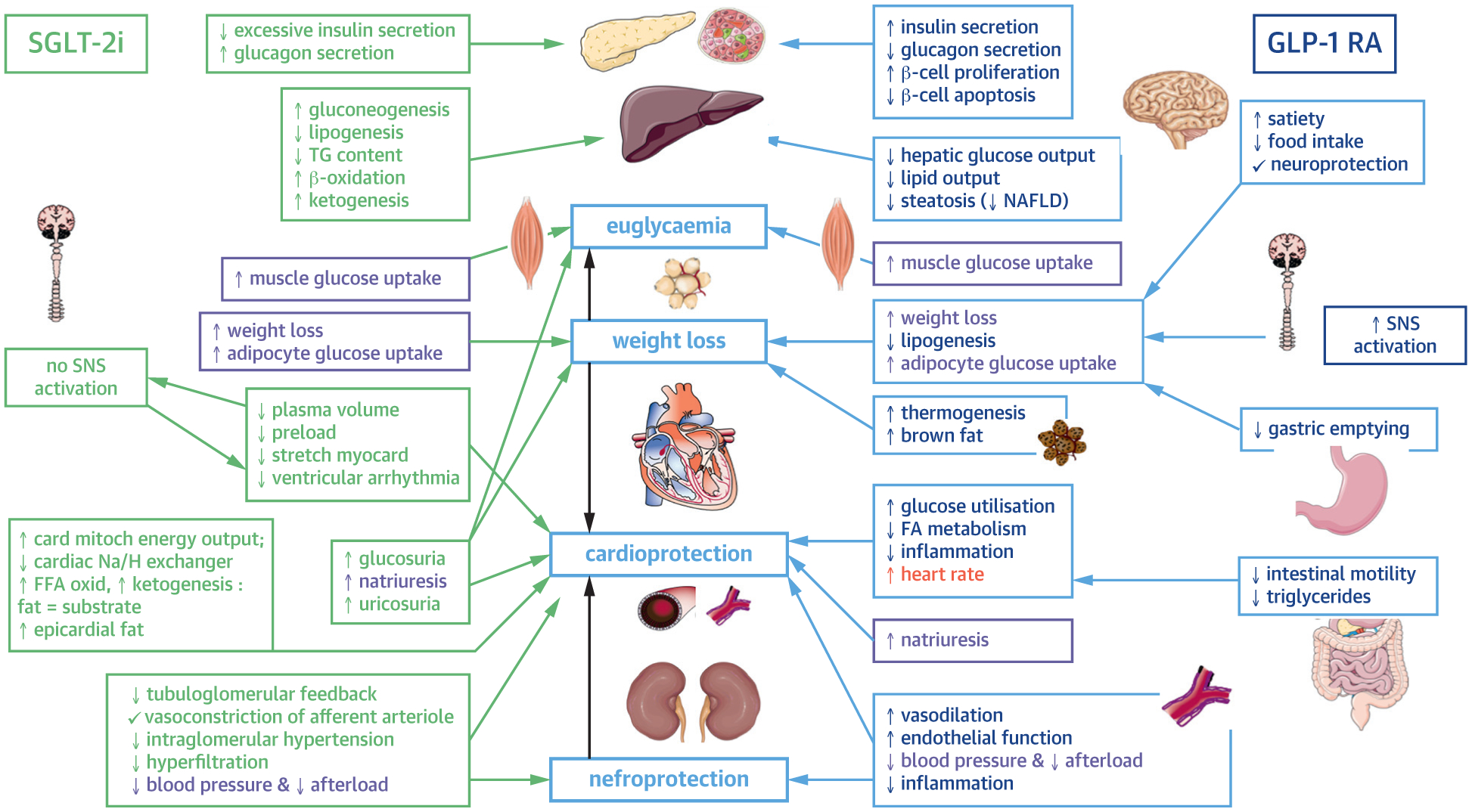
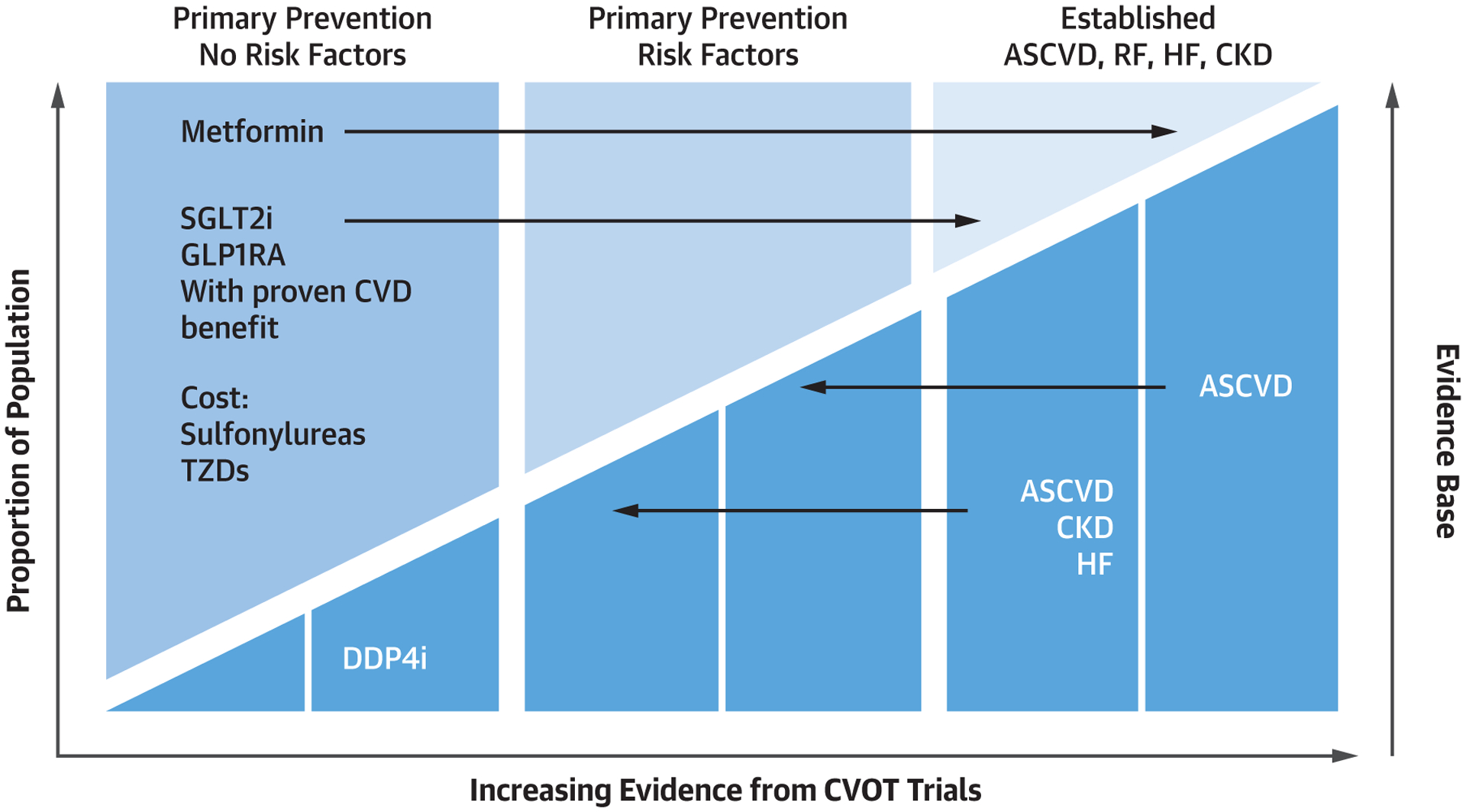
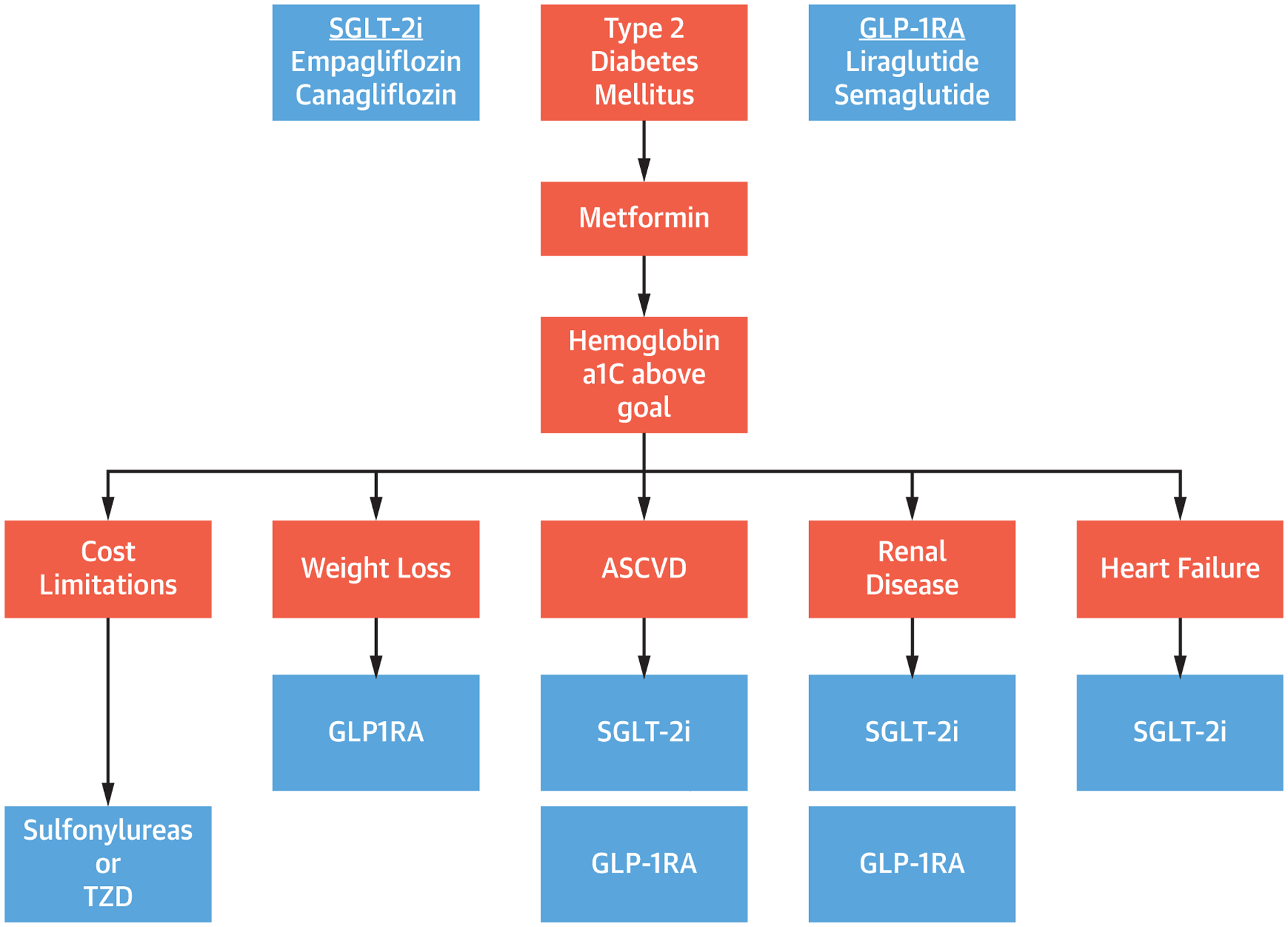
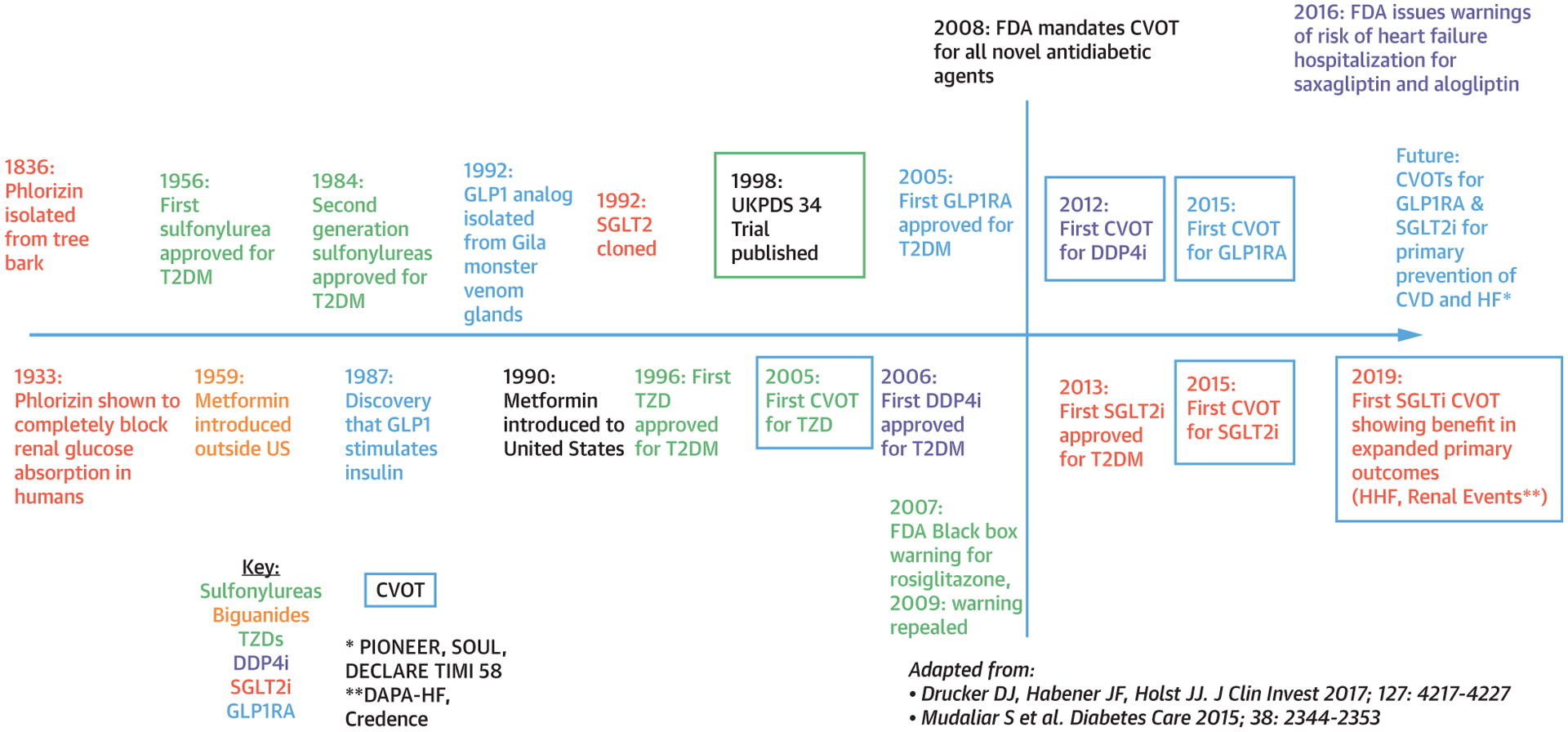
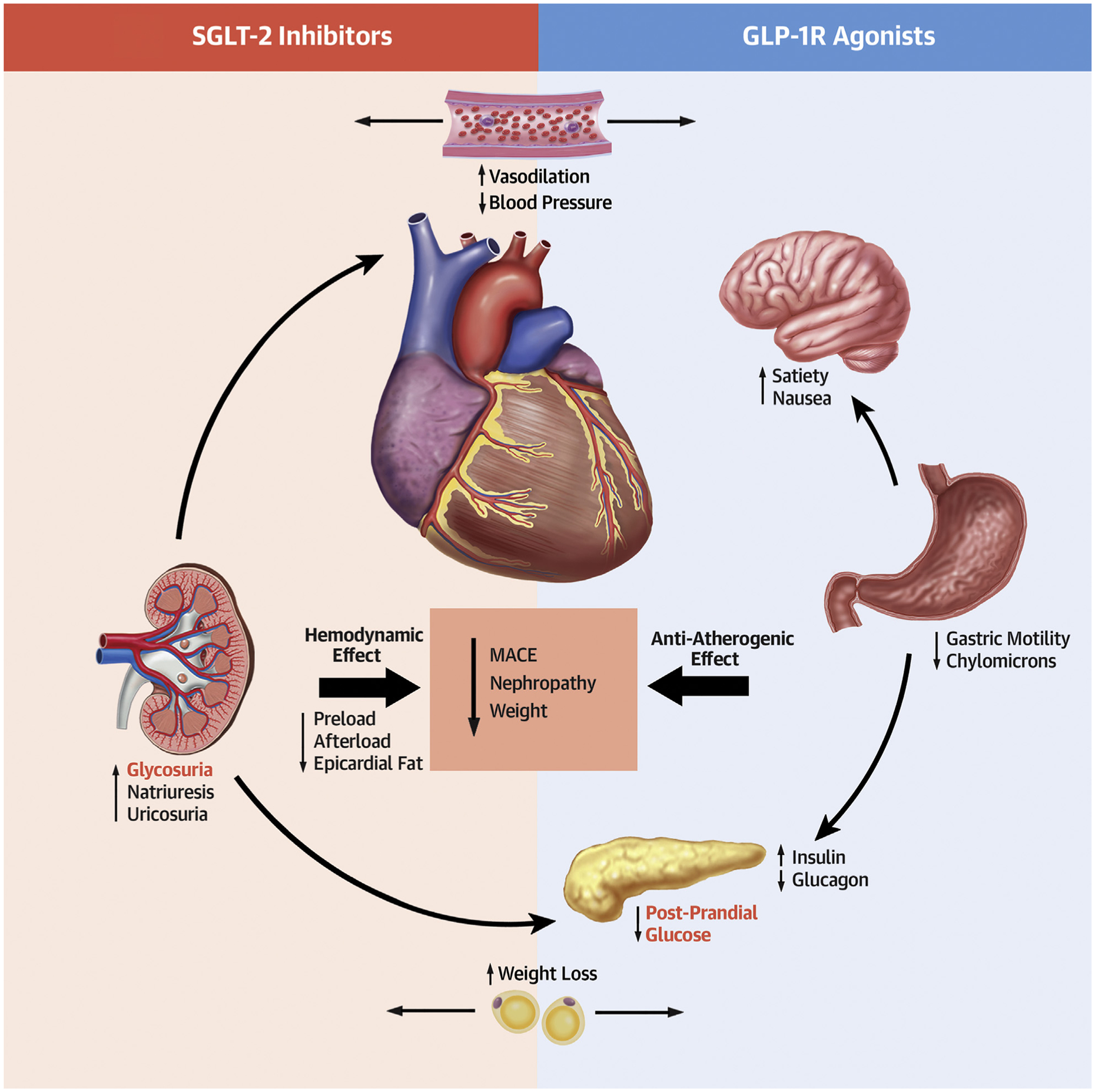
Given the intersection between diabetes mellitus and cardiovascular disease (CVD), pharmacologic agents used to treat type 2 diabetes mellitus must show cardiovascular safety. Comorbid conditions, including heart failure and chronic kidney disease, are increasingly prevalent in patients with diabetes; therefore, they also play a large role in drug safety. Although biguanides, sulfonylurea, glitazones, and dipeptidyl peptidase 4 inhibitors have variable effects on cardiovascular events, sodium glucose cotransporter 2 inhibitors and glucagon-like peptide 1 receptor agonists have consistently shown safety and reduction in cardiovascular events in patients with established CVD. These medications are becoming essential tools for cardioprotection for patients with diabetes and CVD. They may also have roles in primary prevention and renal protection. This paper will review the cardiovascular impact, adverse effects, and possible mechanisms of action of pharmacologic agents used to treat patients with type 2 diabetes.
Keywords: cardiovascular outcomes trials; diabetes drugs; type 2 diabetes.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Gilbert RE, Krum H. Heart failure in diabetes: effects of anti-hyperglycaemic drug therapy. Lancet 2015;385:2107–17. - PubMed
-
- McMurray JJ, Packer M, Desai AS, et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014;371: 993–1004. - PubMed
-
- ADVANCE Collaborative Group, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med 2008; 358:2560–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
