

Circulating Tumor DNA Analysis: Clinical Implications for Colorectal Cancer Patients. A Systematic Review
- PMID: 32328554
- PMCID: PMC7050033
- DOI: 10.1093/jncics/pkz042
Circulating Tumor DNA Analysis: Clinical Implications for Colorectal Cancer Patients. A Systematic Review
Abstract
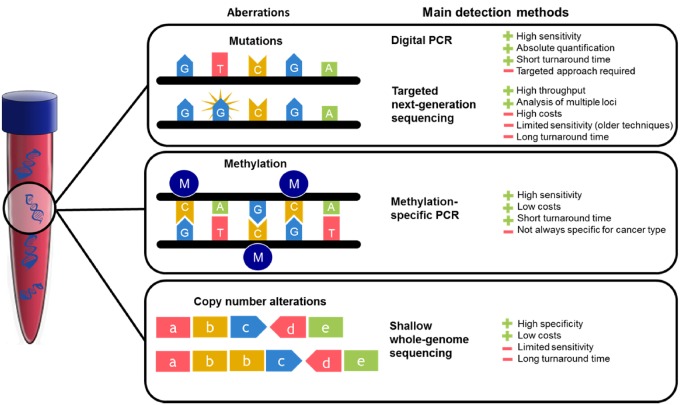
Background: Liquid biopsies could improve diagnosis, prognostication, and monitoring of colorectal cancer (CRC). Mutation, chromosomal copy number alteration, and methylation analysis in circulating tumor DNA (ctDNA) from plasma or serum has gained great interest. However, the literature is inconsistent on preferred candidate markers, hampering a clear direction for further studies and clinical translation. This review assessed the potential of ctDNA analysis for clinical utility.
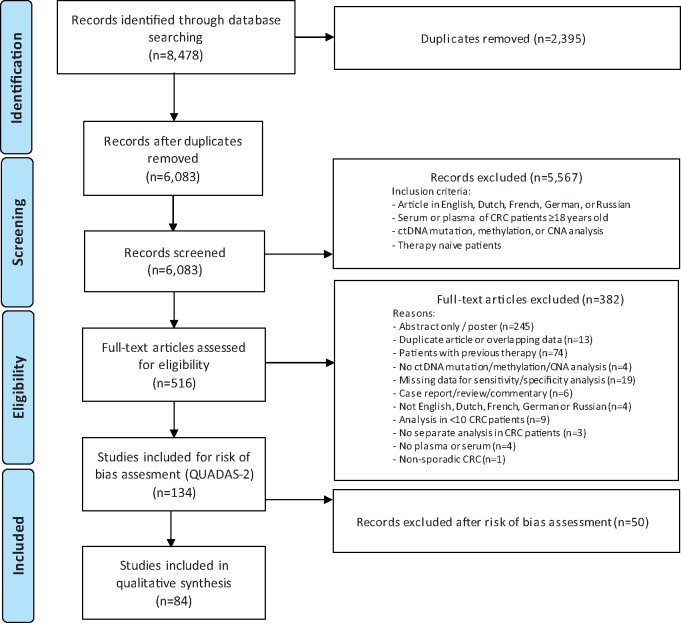
Methods: A systematic review according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines was conducted up to December 3, 2018, followed by methodological quality assessment. Primary endpoints were accuracy for detection, prognostication, and monitoring.
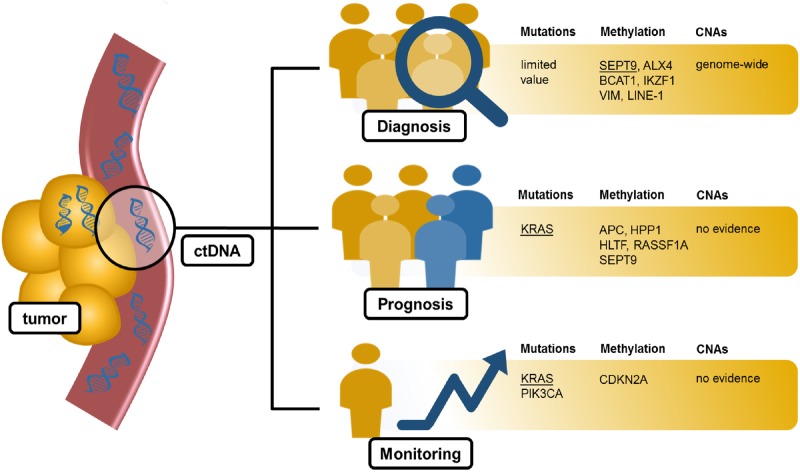
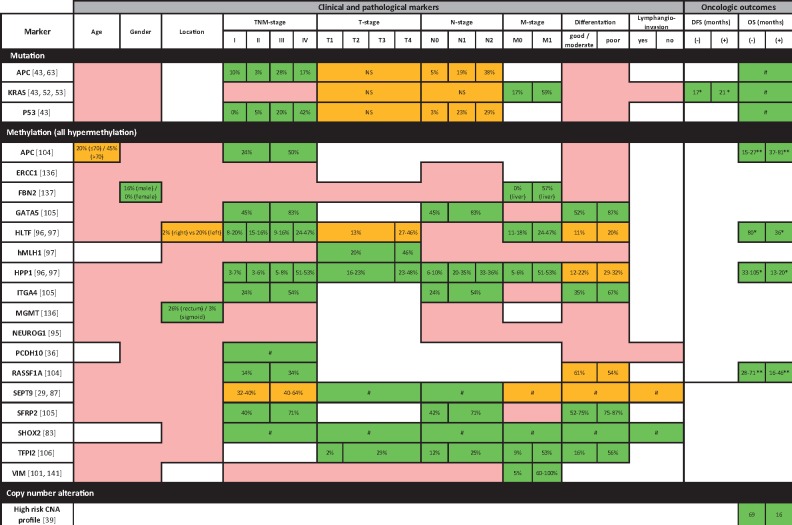
Results: Eighty-four studies were included. For CRC detection, sensitivity was 75% using ctDNA mutation analysis and up to 96% using copy number analysis. Septin 9 (SEPT9) hypermethylation analysis showed sensitivities of 100% and specificities of 97%. Regarding prognostication, ctDNA KRAS mutations were associated with oncological outcome and could predict response to anti-epidermal growth factor receptor therapy. For monitoring, sequential ctDNA KRAS mutation analysis showed promise for detection of relapses or therapy resistance.
Conclusions: This comprehensive overview of ctDNA candidate markers demonstrates SEPT9 methylation analysis to be promising for CRC detection, and KRAS mutation analysis could assist in prognostication and monitoring. Prospective evaluation of marker panels in clinical decision making should bring ctDNA analysis into practice.
© The Author(s) 2019. Published by Oxford University Press.
Figures
References
-
- Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49(6):1374–1403. - PubMed
-
- Siegel RL, Miller KD, Jemal A.. Cancer statistics, 2016. CA Cancer J Clin. 2016;66(1):7–30. - PubMed
-
- Brenner H, Kloor M, Pox CP.. Colorectal cancer. Lancet. 2014;383(9927):1490–1502. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous