

Early and Midterm Outcomes of Open and Endovascular Revascularization of Chronic Mesenteric Ischemia
- PMID: 32328781
- PMCID: PMC7326829
- DOI: 10.1007/s00268-020-05513-2
Early and Midterm Outcomes of Open and Endovascular Revascularization of Chronic Mesenteric Ischemia
Abstract
Background: Revascularization strategies for chronic mesenteric ischemia (CMI) include open (OR) and endovascular (ER) modalities. The primary objective of this study was to analyze the safety and effectiveness of OR and ER and the impact of clinical and morphological variables on early and midterm outcomes in a consecutive series of CMI patients in a tertiary referral center.
Patients and methods: From 2004 to 2017, all CMI patients treated with OR and ER were retrospectively identified. Patient records, preoperative imaging, as well as peri- and postoperative outcomes were analyzed. Univariable and multivariable analysis was performed to identify clinical or morphological variables affecting reintervention rates within 2 years.
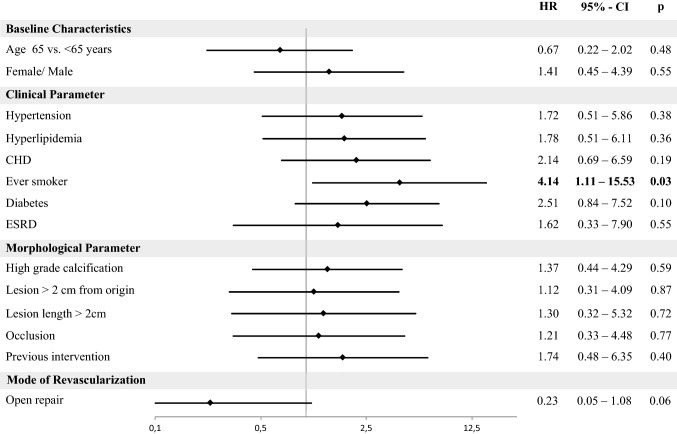
Results: In total, 63 patients (33% male; mean age 71, range 60-76 years) were treated by ER (41 patients) or OR (22 patients) for CMI. Mean follow-up was 26 (10-71) months. 30-day mortality was 0.0% after ER and 4.5% after OR (p = 0.069); 30-day morbidity was 9.8% vs. 31.8%, respectively (p = 0.030). Length of stay was significantly longer after OR (14 vs. 4 days; p < 0.001). Freedom from reintervention rate after 2 years was 82% after OR and 73% after ER (p = 0.14). Overall survival did not differ after 2 years (OR 85% vs. ER 86%; p = 0.35). Multivariable analysis revealed that smoking was associated with higher risk of reintervention (hazard ratio, HR: 4.14; 95% confidence interval, CI 1.11-15.53; p = 0.03). Additionally, a nonsignificant trend of lower reintervention rates after OR was detected (HR 0.23 95% CI 0.05-1.08; p = 0.06).
Conclusion: Due to a lower invasiveness, despite the higher reintervention rate, an "endovascular first" strategy is justified and recommended.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Comment in
-
Letter to the Editor: Early and Midterm Outcomes of Open and Endovascular Revascularization of Chronic Mesenteric Ischemia.World J Surg. 2022 Jul;46(7):1806-1807. doi: 10.1007/s00268-021-06023-5. Epub 2021 Mar 6. World J Surg. 2022. PMID: 33677648 No abstract available.
References
-
- White CJ. Chronic mesenteric ischemia: diagnosis and management. Prog Cardiovasc Dis. 2011;54:36–40. - PubMed
-
- Boley SJ, Brandt LJ, Veith FJ. Ischemic disorders of the intestines. Curr Probl Surg. 1978;15:1–85. - PubMed
-
- Boley SJ, Brandt LJ, Sammartano RJ. History of mesenteric ischemia. The evolution of a diagnosis and management. Surg Clin N Am. 1997;77:275–288. - PubMed
-
- Clair DG, Beach JM. Mesenteric ischemia. N Engl J Med. 2016;374:959–968. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
