

Ventilator Triage Policies During the COVID-19 Pandemic at U.S. Hospitals Associated With Members of the Association of Bioethics Program Directors
- PMID: 32330224
- PMCID: PMC7207244
- DOI: 10.7326/M20-1738
Ventilator Triage Policies During the COVID-19 Pandemic at U.S. Hospitals Associated With Members of the Association of Bioethics Program Directors
Abstract
Background: The coronavirus disease 2019 pandemic has or threatens to overwhelm health care systems. Many institutions are developing ventilator triage policies.
Objective: To characterize the development of ventilator triage policies and compare policy content.
Design: Survey and mixed-methods content analysis.
Setting: North American hospitals associated with members of the Association of Bioethics Program Directors.
Participants: Program directors.
Measurements: Characteristics of institutions and policies, including triage criteria and triage committee membership.
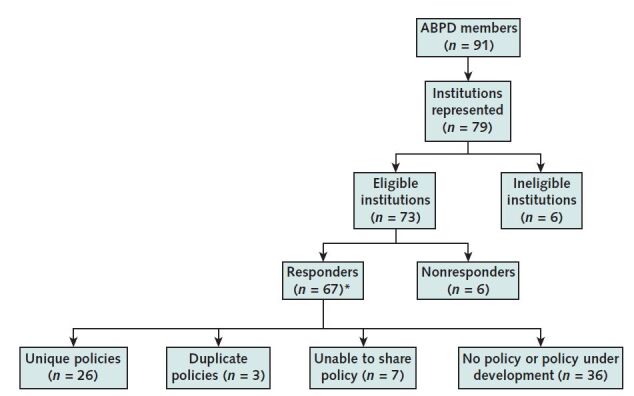
Results: Sixty-seven program directors responded (response rate, 91.8%); 36 (53.7%) hospitals did not yet have a policy, and 7 (10.4%) hospitals' policies could not be shared. The 29 institutions providing policies were relatively evenly distributed among the 4 U.S. geographic regions (range, 5 to 9 policies per region). Among the 26 unique policies analyzed, 3 (11.3%) were produced by state health departments. The most frequently cited triage criteria were benefit (25 policies [96.2%]), need (14 [53.8%]), age (13 [50.0%]), conservation of resources (10 [38.5%]), and lottery (9 [34.6%]). Twenty-one (80.8%) policies use scoring systems, and 20 of these (95.2%) use a version of the Sequential Organ Failure Assessment score. Among the policies that specify the triage team's composition (23 [88.5%]), all require or recommend a physician member, 20 (87.0%) a nurse, 16 (69.6%) an ethicist, 8 (34.8%) a chaplain, and 8 (34.8%) a respiratory therapist. Thirteen (50.0% of all policies) require or recommend that those making triage decisions not be involved in direct patient care, but only 2 (7.7%) require that their decisions be blinded to ethically irrelevant considerations.
Limitation: The results may not be generalizable to institutions without academic bioethics programs.
Conclusion: Over one half of respondents did not have ventilator triage policies. Policies have substantial heterogeneity, and many omit guidance on fair implementation.
Primary funding source: None.
Figures
References
-
- Rosen R. I'm a doctor on the front lines of coronavirus. We've thrown out the rule book. Forward. 3 April 2020. Accessed at https://forward.com/opinion/443033/im-a-doctor-on-the-front-lines-of-tre.... on 8 April 2020.
-
- McCoy K, Wagner D. Which coronavirus patients will get life-saving ventilators? Guidelines show how hospitals in NYC, US will decide. USA Today. 4 April 2020. Accessed at www.usatoday.com/story/news/2020/04/04/coronavirus-ventilator-shortages-.... on 8 April 2020.
-
- Parshley L. You can't use ventilators without sedatives. Now the US is running out of those, too. Vox. 6 April 2020. Accessed at www.vox.com/2020/4/6/21209589/coronavirus-medicine-ventilators-drug-shor.... on 8 April 2020.
-
- Hick JL, Barbera JA, Kelen GD. Refining surge capacity: conventional, contingency, and crisis capacity. Disaster Med Public Health Prep. 2009;3:S59-67. [PMID: 19349869] doi:10.1097/DMP.0b013e31819f1ae2. - PubMed
-
- Institute of Medicine. Guidance for Establishing Crisis Standards of Care for Use in Disaster Situations: A Letter Report. National Academies Pr; 2009. [PMID: 25032361] doi:10.17226/12749. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical