

Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal
- PMID: 32331217
- PMCID: PMC7230457
- DOI: 10.3390/jcm9041191
Helmet CPAP to Treat Acute Hypoxemic Respiratory Failure in Patients with COVID-19: A Management Strategy Proposal
Abstract
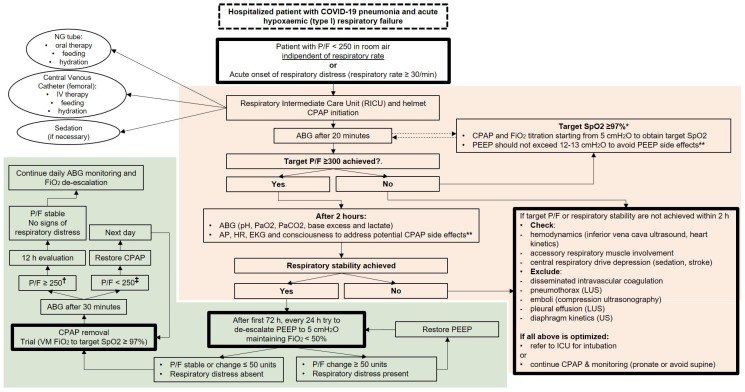
Since the beginning of March 2020, the coronavirus disease 2019 (COVID-19) pandemic has caused more than 13,000 deaths in Europe, almost 54% of which has occurred in Italy. The Italian healthcare system is experiencing a stressful burden, especially in terms of intensive care assistance. In fact, the main clinical manifestation of COVID-19 patients is represented by an acute hypoxic respiratory failure secondary to bilateral pulmonary infiltrates, that in many cases, results in an acute respiratory distress syndrome and requires an invasive ventilator support. A precocious respiratory support with non-invasive ventilation or high flow oxygen should be avoided to limit the droplets' air-dispersion and the healthcare workers' contamination. The application of a continuous positive airway pressure (CPAP) by means of a helmet can represent an effective alternative to recruit diseased alveolar units and improve hypoxemia. It can also limit the room contamination, improve comfort for the patients, and allow for better clinical assistance with long-term tolerability. However, the initiation of a CPAP is not free from pitfalls. It requires a careful titration and monitoring to avoid a delayed intubation. Here, we discuss the rationale and some important considerations about timing, criteria, and monitoring requirements for patients with COVID-19 respiratory failure requiring a CPAP treatment.
Keywords: COVID-19; continuous positive airway pressure; helmet; hypoxia; pneumonia; positive end-expiratory pressure; respiratory failure; severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- World Health Organization COVID-19 Situation in the WHO European Region. [(accessed on 27 March 2020)]; Available online: https://who.maps.arcgis.com/apps/opsdashboard/index.html#/ead3c647565448....
LinkOut - more resources
Full Text Sources
Miscellaneous
