

Pain Neuroscience Education and Physical Therapeutic Exercise for Patients with Chronic Spinal Pain in Spanish Physiotherapy Primary Care: A Pragmatic Randomized Controlled Trial
- PMID: 32331323
- PMCID: PMC7230486
- DOI: 10.3390/jcm9041201
Pain Neuroscience Education and Physical Therapeutic Exercise for Patients with Chronic Spinal Pain in Spanish Physiotherapy Primary Care: A Pragmatic Randomized Controlled Trial
Abstract
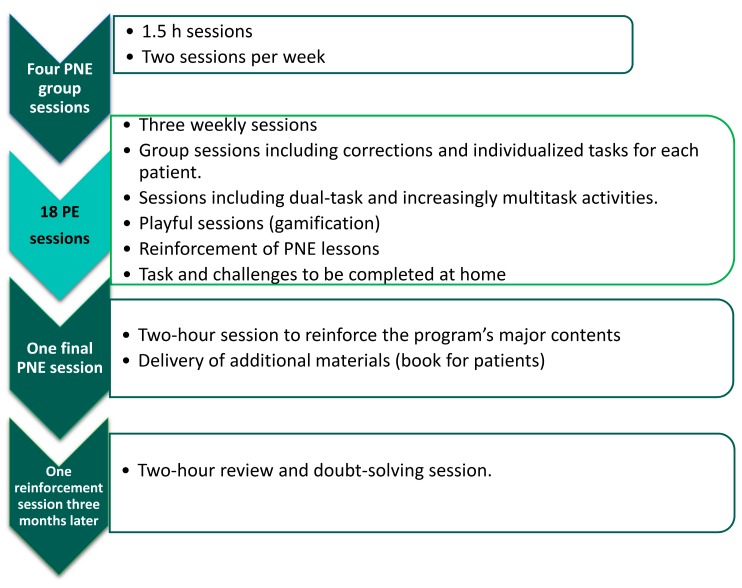
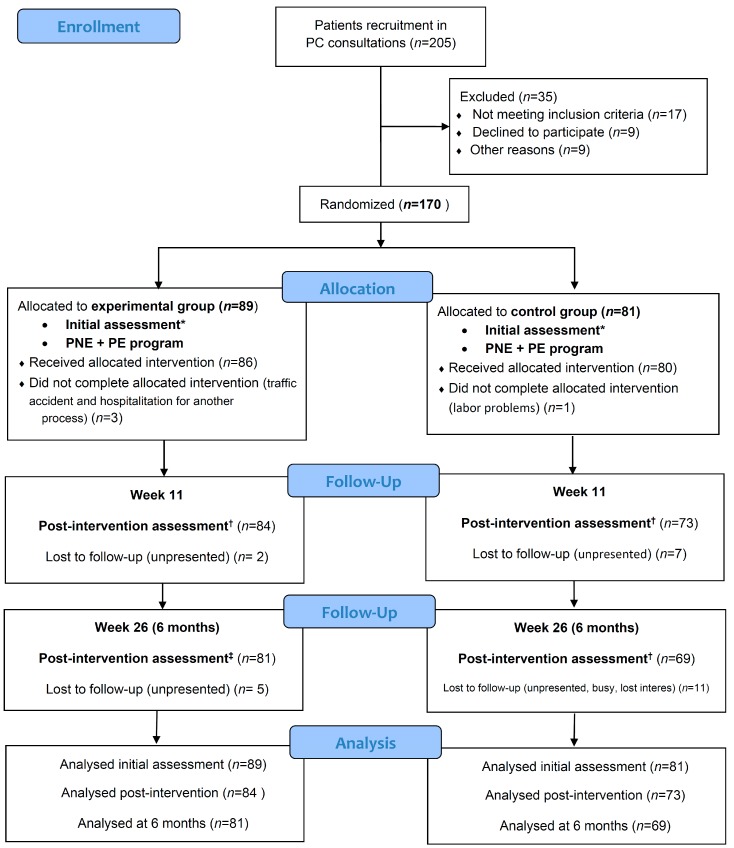
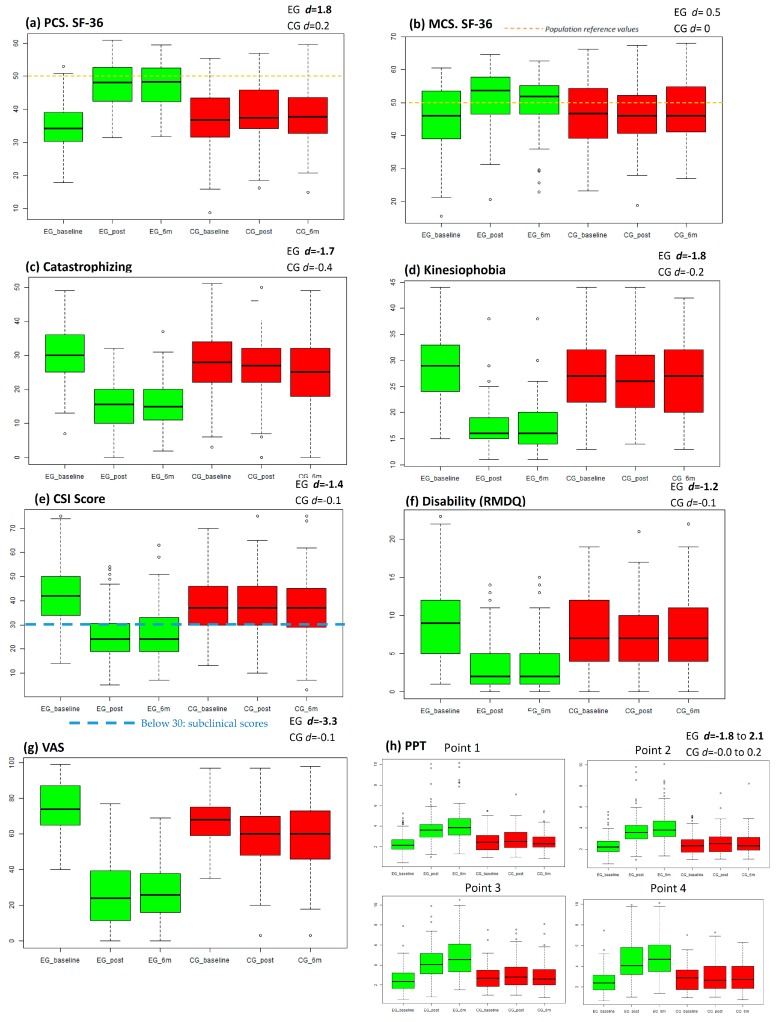
Chronic musculoskeletal pain affects more than 20% of the population, leading to high health care overload and huge spending. The prevalence is increasing and negatively affects both physical and mental health, being one of the leading causes of disability. The most common location is the spine. Most treatments used in the Public Health Services are passive (pharmacological and invasive) and do not comply with current clinical guidelines, which recommend treating pain in primary care (PC) with education and exercise as the first-line treatments. A randomized multicentre clinical trial has been carried out in 12 PC centres. The experimental group (EG) conducted a program of pain neuroscience education (6 sessions, 10 h) and group physical exercise with playful, dual-tasking, and socialization-promoting components (18 sessions in 6 weeks, 18 h), and the control group performed the usual physiotherapy care performed in PC. The experimental treatment improved quality of life (d = 1.8 in physical component summary), catastrophism (d = 1.7), kinesiophobia (d = 1.8), central sensitization (d = 1.4), disability (d = 1.4), pain intensity (d = 3.3), and pressure pain thresholds (d = 2). Differences between the groups (p < 0.001) were clinically relevant in favour of the EG. Improvements post-intervention (week 11) were maintained at six months. The experimental treatment generates high levels of satisfaction.
Keywords: chronic pain; chronic spinal pain; pain neuroscience education; physical exercise; primary care; randomized controlled trial.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- James S.L., Abate D., Abate K.H., Abay S.M., Abbafati C., Abbasi N., Abbastabar H., Abd-Allah F., Abdela J., Abdelalim A., et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Barbaglia G., Adroher N.D., Vilagut G., Bruffaerts R., Bunting B., Caldas de Almeida J.M., Florescu S., de Girolamo G., de Graaf R., Haro J.M., et al. Health conditions and role limitation in three European Regions: A public-health perspective. Gac. Sanit. 2017;31:2–10. doi: 10.1016/j.gaceta.2016.07.008. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
