

Functional arrays of human pluripotent stem cell-derived cardiac microtissues
- PMID: 32332814
- PMCID: PMC7181791
- DOI: 10.1038/s41598-020-62955-3
Functional arrays of human pluripotent stem cell-derived cardiac microtissues
Abstract
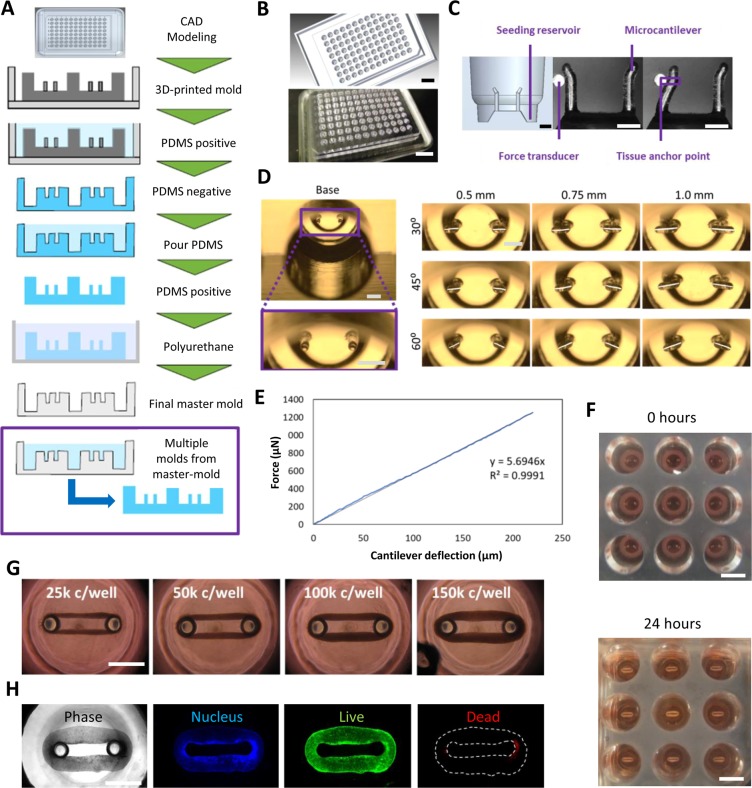
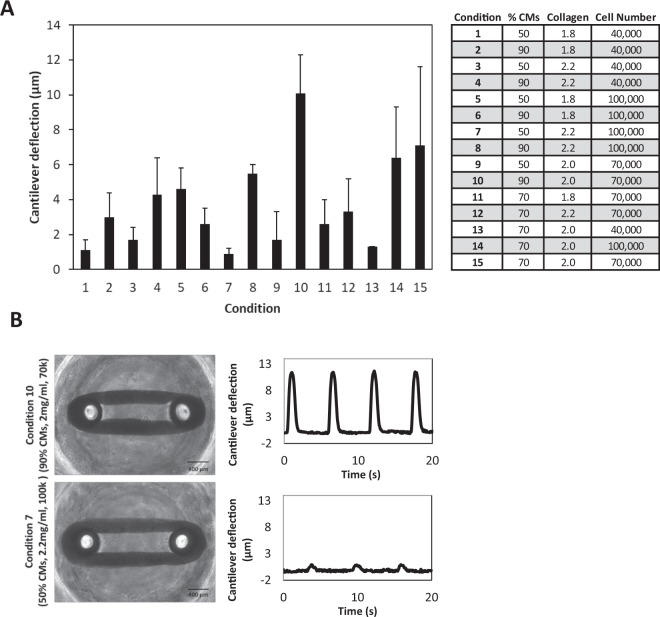
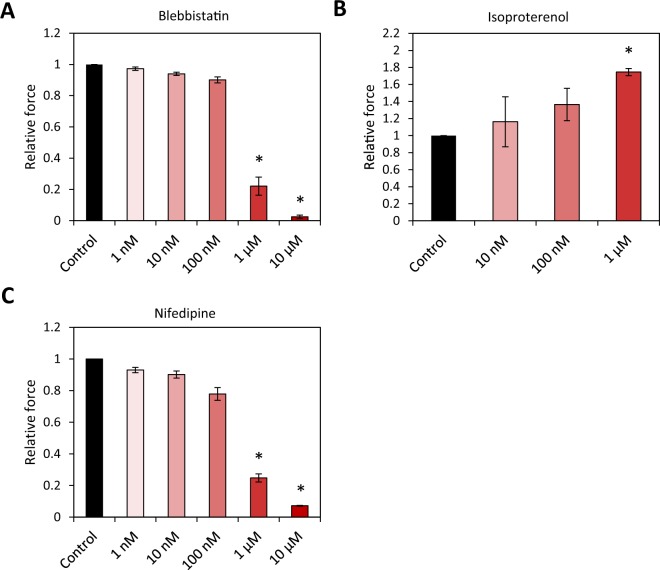
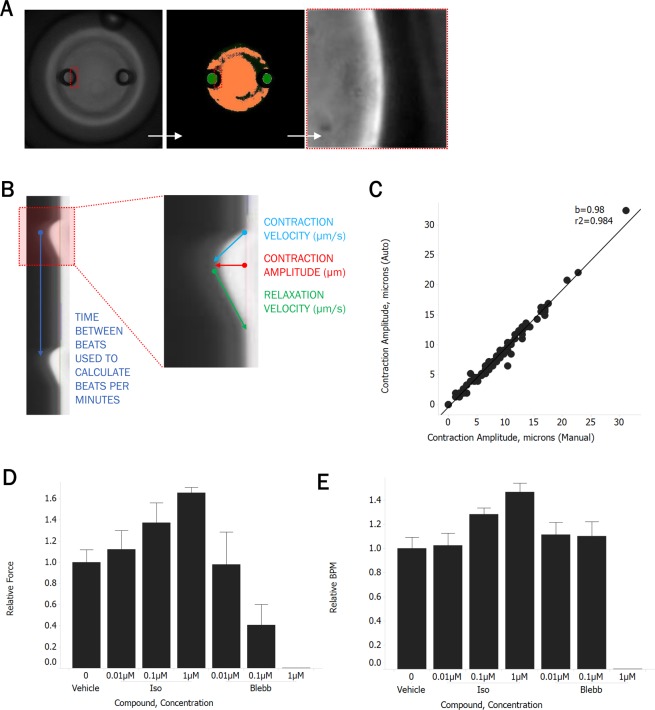
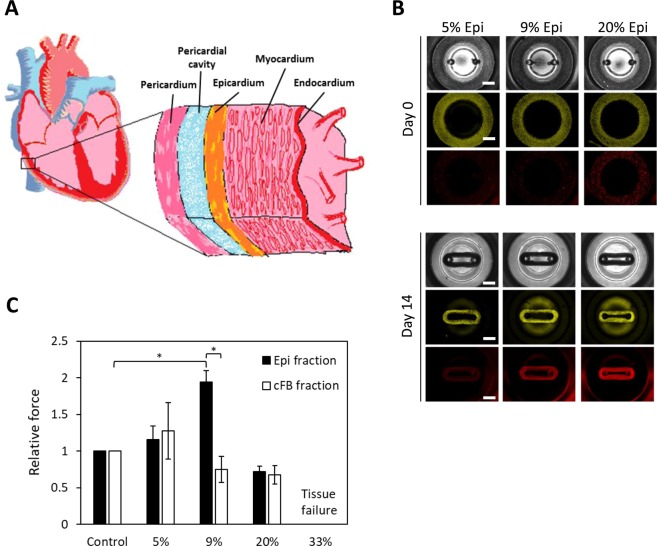
To accelerate the cardiac drug discovery pipeline, we set out to develop a platform that would be capable of quantifying tissue-level functions such as contractile force and be amenable to standard multiwell-plate manipulations. We report a 96-well-based array of 3D human pluripotent stem cell (hPSC)-derived cardiac microtissues - termed Cardiac MicroRings (CaMiRi) - in custom 3D-print-molded multiwell plates capable of contractile force measurement. Within each well, two elastomeric microcantilevers are situated above a circumferential ramp. The wells are seeded with cell-laden collagen, which, in response to the gradual slope of the circumferential ramp, self-organizes around tip-gated microcantilevers to form contracting CaMiRi. The contractile force exerted by the CaMiRi is measured and calculated using the deflection of the cantilevers. Platform responses were robust and comparable across wells, and we used it to determine an optimal tissue formulation. We validated the contractile force response of CaMiRi using selected cardiotropic compounds with known effects. Additionally, we developed automated protocols for CaMiRi seeding, image acquisition, and analysis to enable the measurement of contractile force with increased throughput. The unique tissue fabrication properties of the platform, and the consequent effects on tissue function, were demonstrated upon adding hPSC-derived epicardial cells to the system. This platform represents an open-source contractile force screening system useful for drug screening and tissue engineering applications.
Conflict of interest statement
N.T., M.R., and P.W.Z. are co-inventors on a patent covering the design of cardiac microtissue formation: “Cardiac tissue constructs and methods of fabrication thereof”. N.T. and M.R. are co-inventors on a patent covering the design of microtissue formation: “Compositions and methods for making and using three-dimensional tissue systems”. C.H., P.T., and H.L. are employees of Amgen Inc. Amgen has an interest in cardiac-associated drug discovery and contributed to this study. H.X., M.L.S., and M.E.M. are current employees of A2 Biotherapeutics Inc., and previous employees of Amgen Inc. A2 Biotherapeutics has an interest in cardiac-associated drug discovery. M.R. holds equity in and receives consulting income from TARA Biosystems, a company that uses heart tissues in drug discovery.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
