

Modeling biological and genetic diversity in upper tract urothelial carcinoma with patient derived xenografts
- PMID: 32332851
- PMCID: PMC7181640
- DOI: 10.1038/s41467-020-15885-7
Modeling biological and genetic diversity in upper tract urothelial carcinoma with patient derived xenografts
Abstract
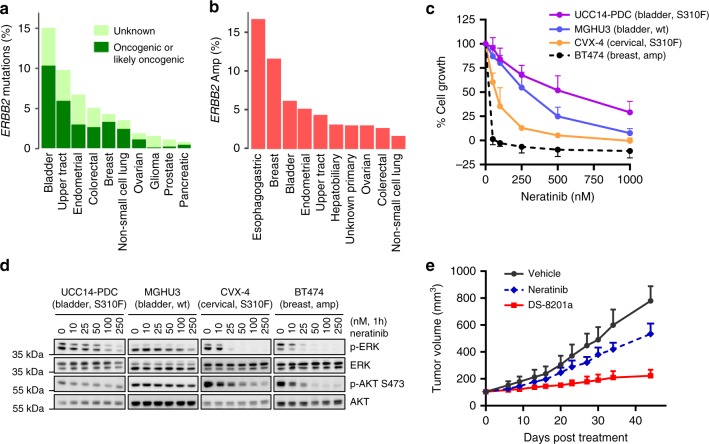
Treatment paradigms for patients with upper tract urothelial carcinoma (UTUC) are typically extrapolated from studies of bladder cancer despite their distinct clinical and molecular characteristics. The advancement of UTUC research is hampered by the lack of disease-specific models. Here, we report the establishment of patient derived xenograft (PDX) and cell line models that reflect the genomic and biological heterogeneity of the human disease. Models demonstrate high genomic concordance with the corresponding patient tumors, with invasive tumors more likely to successfully engraft. Treatment of PDX models with chemotherapy recapitulates responses observed in patients. Analysis of a HER2 S310F-mutant PDX suggests that an antibody drug conjugate targeting HER2 would have superior efficacy versus selective HER2 kinase inhibitors. In sum, the biological and phenotypic concordance between patient and PDXs suggest that these models could facilitate studies of intrinsic and acquired resistance and the development of personalized medicine strategies for UTUC patients.
Conflict of interest statement
M.S. is in the Advisory Board of Bioscience Institute and Menarini Ricerche, received research funds from Puma Biotechnology, Daiichi-Sankio, Targimmune, Immunomedics and Menarini Ricerche, is a co-founder of Medendi Medical Travel and in the past two years he received honoraria from Menarini Ricerche and ADC Pharma. E.J.P. is on the scientific advisory board for Merck. J.J.H. is a consultant of Eisai (RCC Strategic Council) (2018-2019) and received research funds from BostonGene (2019). D.B.S. has served as a consultant and received honoraria from Pfizer, Loxo Oncology, Lilly Oncology, Vivideon Therapeutics, Q.E.D. Therapeutics and Illumina. A.D.S. is in the Advisory Board of Merck and Tesaro, received research funds from R-Pharma, Gilead, Genentech, Boheringer, Puma Biotechnology and Immunomedics. The remaining authors declare no conflicts of interest.
Figures
Comment in
-
Urological Oncology: Bladder, Penis and Urethral Cancer, and Basic Principles of Oncology.J Urol. 2021 Jun;205(6):1821-1823. doi: 10.1097/JU.0000000000001721. Epub 2021 Apr 8. J Urol. 2021. PMID: 33827232 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
