

Bridging repair of the abdominal wall in a rat experimental model. Comparison between uncoated and polyethylene oxide-coated equine pericardium meshes
- PMID: 32332926
- PMCID: PMC7181852
- DOI: 10.1038/s41598-020-63886-9
Bridging repair of the abdominal wall in a rat experimental model. Comparison between uncoated and polyethylene oxide-coated equine pericardium meshes
Abstract
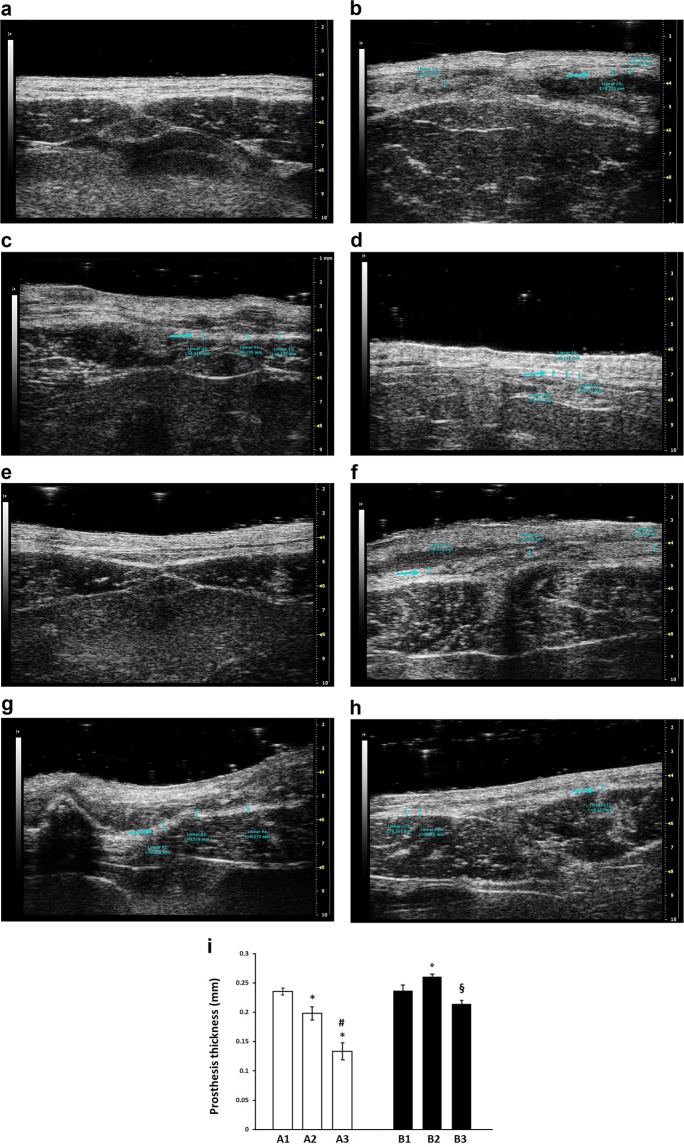
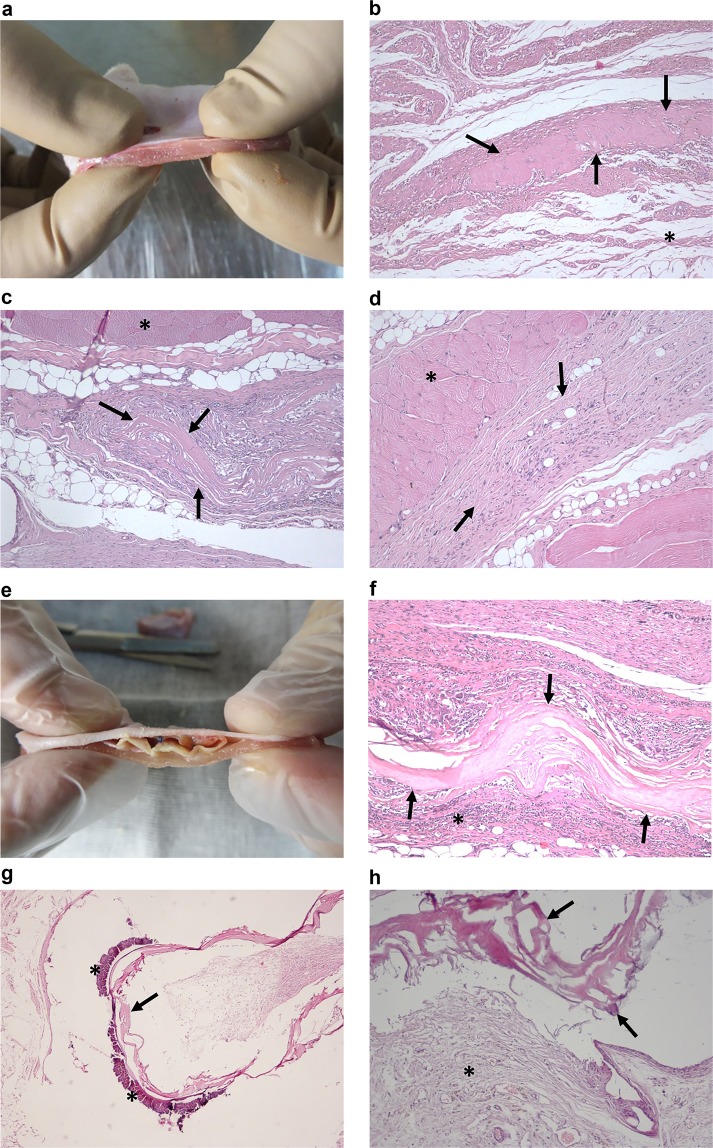
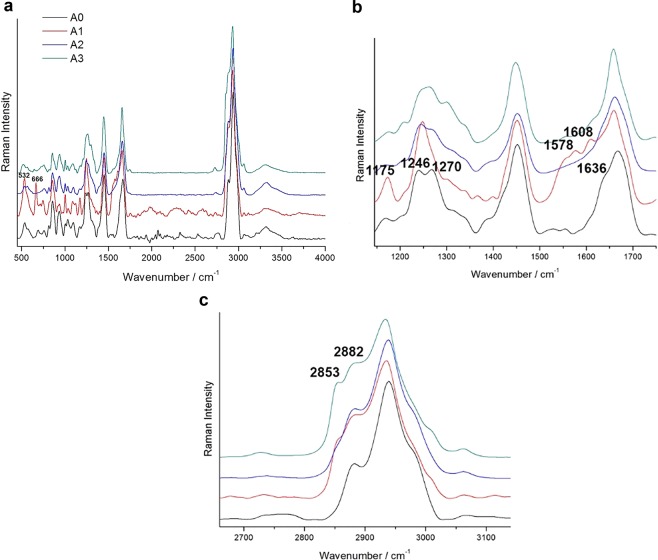
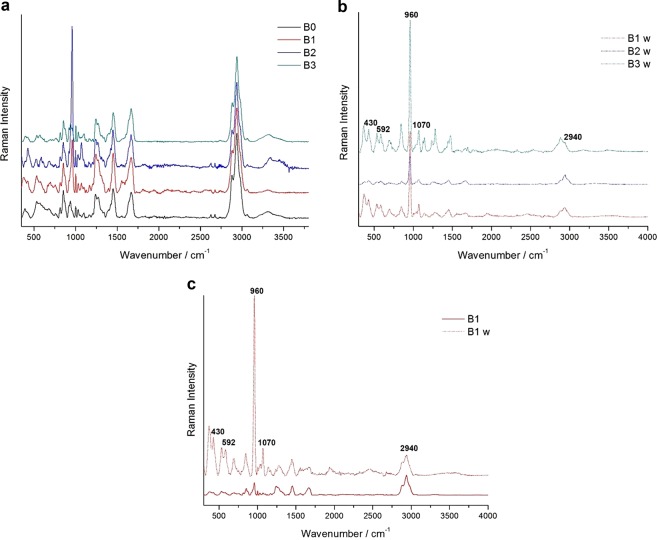
Biological meshes improve the outcome of incisional hernia repairs in infected fields but often lead to recurrence after bridging techniques. Sixty male Wistar rats undergoing the excision of an abdominal wall portion and bridging mesh repair were randomised in two groups: Group A (N = 30) using the uncoated equine pericardium mesh; Group B (N = 30) using the polyethylene oxide (PEO)-coated one. No deaths were observed during treatment. Shrinkage was significantly less common in A than in B (3% vs 53%, P < 0.001). Adhesions were the most common complication and resulted significantly higher after 90 days in B than in A (90% vs 30%, P < 0.01). Microscopic examination revealed significantly (P < 0.05) higher mesh integrity, fibrosis and calcification in B compared to A. The enzymatic degradation, as assessed with Raman spectroscopy and enzyme stability test, affected A more than B. The PEO-coated equine pericardium mesh showed higher resistance to biodegradation compared to the uncoated one. Understanding the changes of these prostheses in a surgical setting may help to optimize the PEO-coating in designing new biomaterials for the bridging repair of the abdominal wall.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Usher FC, Ochsner J, Tuttle LL., Jr. Use of marlex mesh in the repair of incisional hernias. Am. Surg. 1985;24:969–974. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
