

A structured approach to native mitral valve infective endocarditis: Is repair better than replacement?
- PMID: 32333009
- PMCID: PMC7453034
- DOI: 10.1093/ejcts/ezaa079
A structured approach to native mitral valve infective endocarditis: Is repair better than replacement?
Abstract
Objectives: Mitral valve repair in native active infective endocarditis is technically challenging. The survival benefit over valve replacement is poorly established and possibly absent because of the high risk of repair failure and reoperation. In this study, we explore the results of our structured approach in these patients.
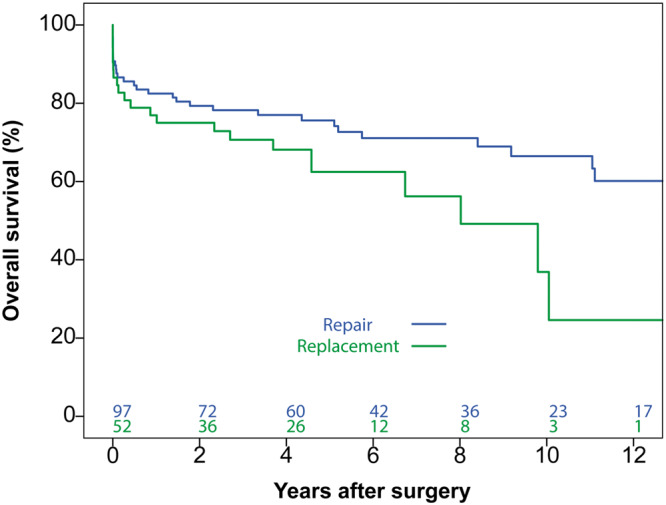
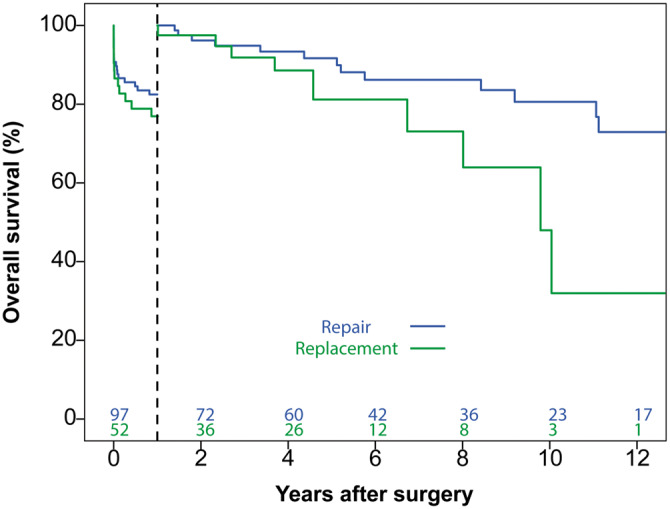
Methods: Between January 2000 and January 2017, 149 patients underwent surgery for native mitral infective endocarditis. Among them, 97 (66%) patients underwent valve repair and 52 (34%) underwent valve replacement. Our structured approach consisted of early surgery, radical resection of infected tissue, liberal use of prosthetic materials and 'patch' repair techniques. A critical assessment of expected repair durability was made intraoperatively and repair was not performed if concerns of long-term durability existed. To study the effects of valve repair on overall survival, landmark analysis was performed.
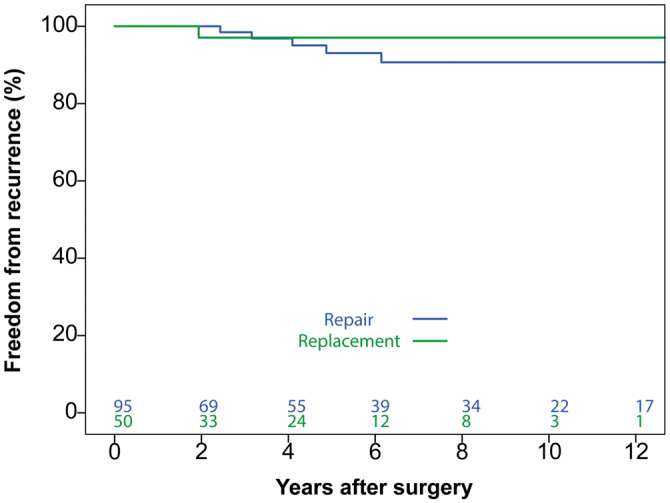
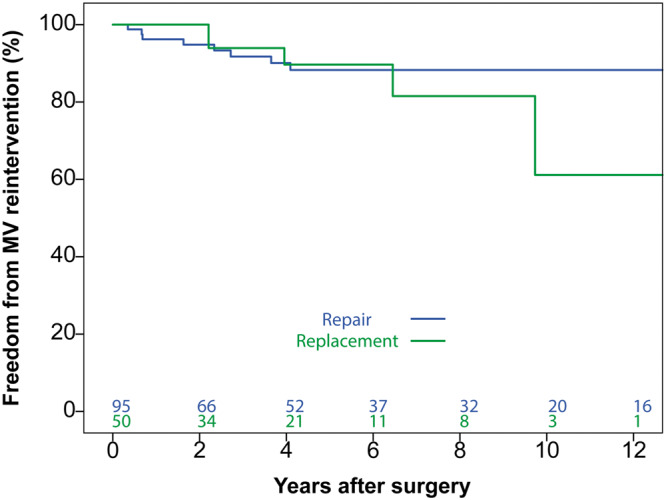
Results: In-hospital mortality was 15.4% (14 repair vs 9 replacement patients; P = 0.642). There were no residual infective endocarditis cases or early reoperations. On Cox proportional hazards analysis, valve replacement was not inferior to repair within 1-year post-surgery [hazard ratio (HR) 1.134, 95% confidence interval (CI) 0.504-2.540; P = 0.76]. Beyond 1 year post-surgery, replacement was associated with decreased survival (HR 2.534, 95% CI 1.002-6.406; P = 0.049). There were no differences in freedom from recurrent infective endocarditis (P = 0.47) and mitral valve reintervention (P = 0.52).
Conclusions: Active mitral valve endocarditis remains a complex disease with significant early and late morbidity and mortality. A structured approach allows valve repair in two-thirds of patients. Clinical results could be improved by focussing on early surgery, prior to extensive valve destruction, to enable durable repairs and improve late outcomes.
Keywords: Infective endocarditis; Mitral valve repair; Mitral valve replacement.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
References
-
- Dreyfus G, Serraf A, Jebara VA, Deloche A, Chauvaud S, Couetil JP. et al. Valve repair in acute endocarditis. Ann Thorac Surg 1990;49:706–11; discussion 12–3. - PubMed
-
- Feringa HH, Shaw LJ, Poldermans D, Hoeks S, van der Wall EE, Dion RA. et al. Mitral valve repair and replacement in endocarditis: a systematic review of literature. Ann Thorac Surg 2007;83:564–70. - PubMed
-
- Liu JZ, Li XF, Miao Q, Zhang CJ.. Surgical treatment of active native mitral infective endocarditis: a meta-analysis of current evidence. J Chin Med Assoc 2018;81:147–54. - PubMed
-
- Perrotta S, Frojd V, Lepore V, Schersten H, Jeppsson A, Svensson G.. Surgical treatment for isolated mitral valve endocarditis: a 16-year single-centre experience. Eur J Cardiothorac Surg 2018;53:576–81. - PubMed
-
- Toyoda N, Itagaki S, Egorova NN, Tannous H, Anyanwu AC, El-Eshmawi A. et al. Real-world outcomes of surgery for native mitral valve endocarditis. J Thorac Cardiovasc Surg 2017;154:1906–12.e9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
