

Prevalence, predictors, and prognosis of symptomatic intracranial stenosis in patients with transient ischaemic attack or minor stroke: a population-based cohort study
- PMID: 32333899
- PMCID: PMC7116132
- DOI: 10.1016/S1474-4422(20)30079-X
Prevalence, predictors, and prognosis of symptomatic intracranial stenosis in patients with transient ischaemic attack or minor stroke: a population-based cohort study
Abstract
Background: Symptomatic intracranial stenosis was perceived to convey a high risk of recurrent stroke, but two previous trials (SAMMPRIS and VISSIT) did not show superiority of intracranial stenosis stenting over intensive medical management alone. These findings were partly due to a lower than expected risk of recurrent stroke without stenting, possibly reflecting the young age of recruits (median age <60 years), and raise questions about generalisability to routine clinical practice. We therefore studied the age-specific prevalence, predictors, and prognosis of symptomatic intracranial stenosis in a population-based cohort of patients with transient ischaemic attack and minor stroke on intensive medical management.
Methods: The Oxford Vascular Study (OXVASC) is a prospective incidence cohort study of all vascular events in a population of 92 728 people residing in Oxfordshire, UK. All patients, irrespective of age, with transient ischaemic attack and minor ischaemic stroke occurring between March 1, 2011, and March 1, 2018 (follow-up to Sept 28, 2018), were ascertained with multiple methods, including assessment in a dedicated daily emergency clinic and daily review of all hospital admissions. Imaging was by MR angiography of the intracranial and cervicocranial arteries, by CT angiography if MR angiography was contraindicated, and by transcranial Doppler and carotid ultrasound if CT angiography was contraindicated. All patients received intensive medical treatment without stenting, and those with intracranial vascular imaging were analysed in our study, which assessed the age-specific prevalence of 50-99% intracranial stenosis and the associated stroke risk of 50-99% and 70-99% stenosis (adjusted for age and vascular risk factors) during follow-up to Sept 28, 2018.
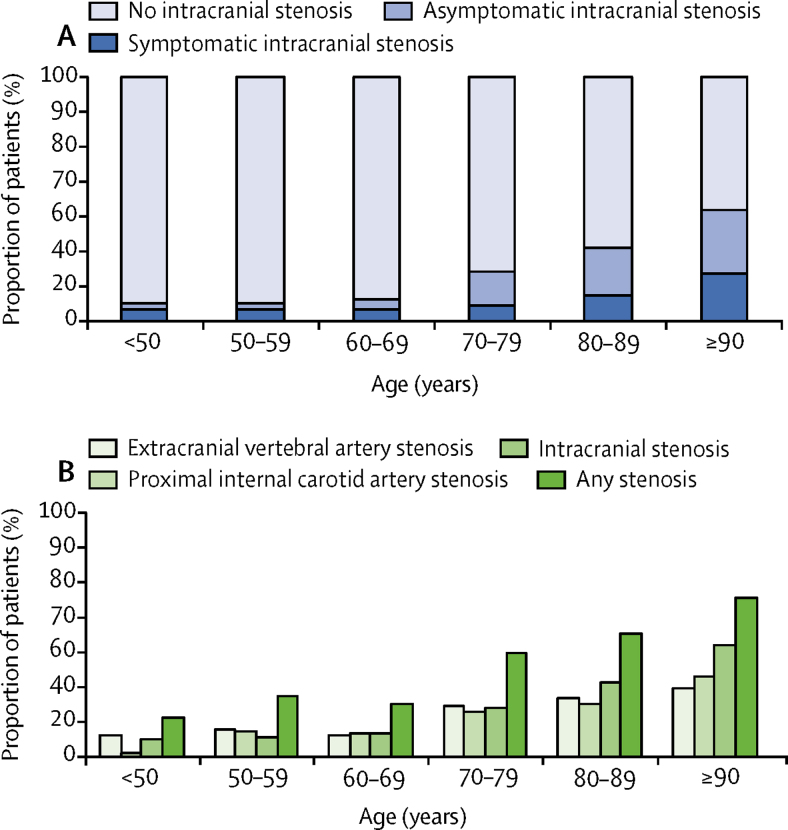
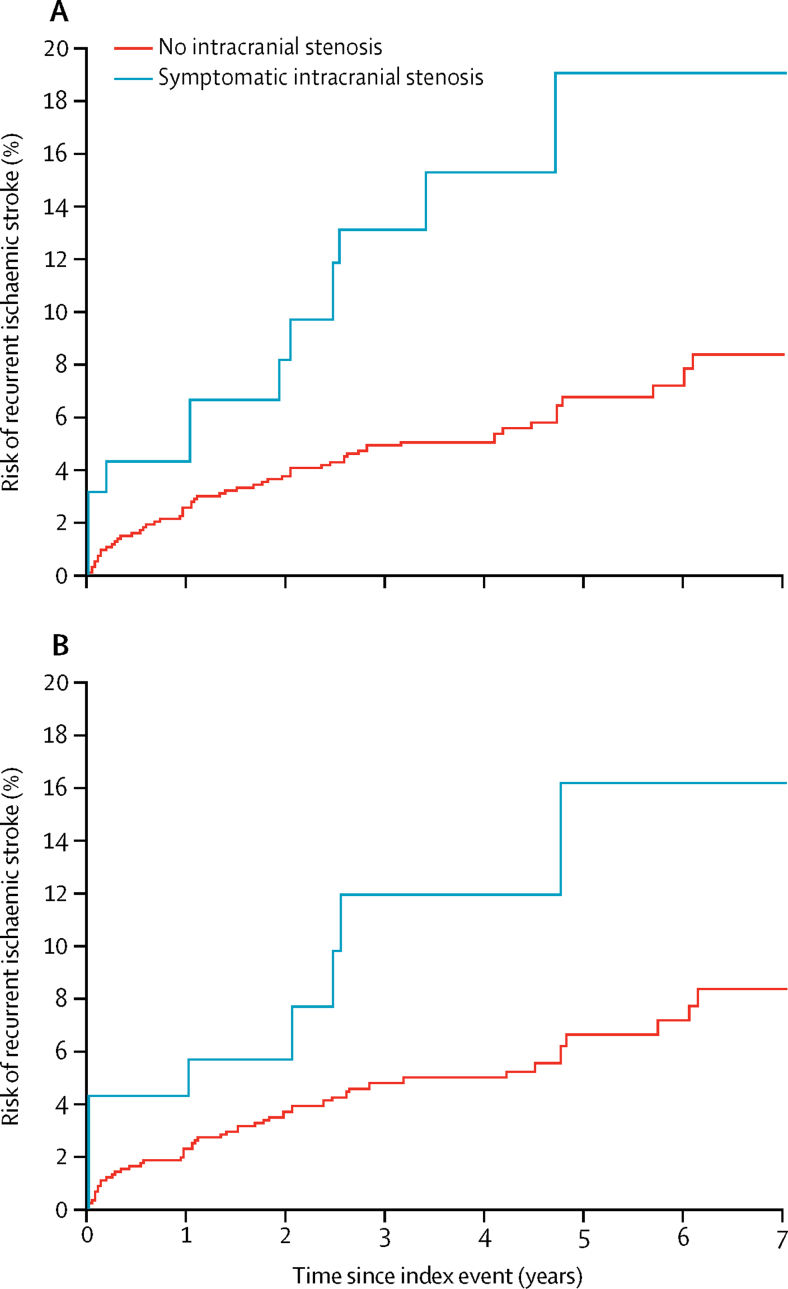
Findings: Of 1368 eligible patients with intracranial vascular imaging, 241 (17·6%) had 385 50-99% symptomatic or asymptomatic intracranial stenosis. The prevalence of symptomatic 50-99% intracranial stenosis increased from 29 (4·9%) of 596 at younger than 70 years to 10 (19·6%) of 51 at 90 years or older (ptrend<0·0001). Of 94 patients with 50-99% symptomatic intracranial stenosis, 14 (14·9%) had recurrent strokes (12 ischaemic and two haemorrhagic) during a median follow-up of 2·8 years (IQR 1·5-4·6). Although symptomatic intracranial stenosis conveyed an increased risk of ischaemic stroke compared with no intracranial stenosis (adjusted hazard ratio 1·43, 95% CI 1·04-1·96), the risk of same-territory ischaemic stroke in patients with 70-99% symptomatic intracranial stenosis tended to be less than those reported in the non-stenting groups of the previous trials (1-year risk 5·6% [95% CI 0·0-13·0] vs 9·4% [3·1-20·7] in VISSIT; 2-year risk 5·6% [0·0-13·0] vs 14·1% [10·1-19·4] in SAMMPRIS).
Interpretation: The prevalence of 50-99% symptomatic intracranial stenosis increases steeply with age in predominantly Caucasian patients with transient ischaemic attack and minor ischaemic stroke. However, the risk of recurrent stroke on intensive medical treatment of symptomatic intracranial stenosis is consistent with the two previous randomised controlled trials in younger cohorts, supporting the generalisability of the trial results to routine practice.
Funding: Wellcome Trust, Wolfson Foundation, British Heart Foundation, National Institute for Health Research, National Institute for Health Research Oxford Biomedical Research Centre, Association of British Neurologists.
Copyright © 2020 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Intensive medical management of intracranial arterial stenosis.Lancet Neurol. 2020 May;19(5):371-373. doi: 10.1016/S1474-4422(20)30100-9. Lancet Neurol. 2020. PMID: 32333887 No abstract available.
References
-
- Amarenco P, Lavallée PC, Monteiro Tavares L. Five-year risk of stroke after TIA or minor ischemic stroke. N Engl J Med. 2018;378:2182–2190. - PubMed
-
- Suwanwela NC, Chutinetr A. Risk factors for atherosclerosis of cervicocerebral arteries: intracranial versus extracranial. Neuroepidemiology. 2003;22:37–40. - PubMed
-
- Huang YN, Gao S, Li SW. Vascular lesions in Chinese patients with transient ischemic attacks. Neurology. 1997;48:524–525. - PubMed
-
- Liu HM, Tu YK, Yip PK, Su CT. Evaluation of intracranial and extracranial carotid steno-occlusive diseases in Taiwan Chinese patients with MR angiography: preliminary experience. Stroke. 1996;27:650–653. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
