

Dispensations of benzodiazepines, z-hypnotics, and gabapentinoids to patients receiving opioid agonist therapy; a prospective cohort study in Norway from 2013 to 2017
- PMID: 32334602
- PMCID: PMC7183604
- DOI: 10.1186/s12913-020-05195-5
Dispensations of benzodiazepines, z-hypnotics, and gabapentinoids to patients receiving opioid agonist therapy; a prospective cohort study in Norway from 2013 to 2017
Abstract
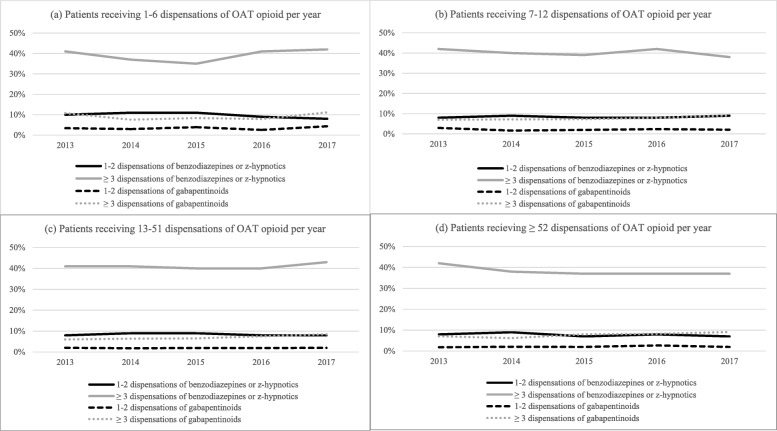
Background: Dispensations of benzodiazepines, z-hypnotics, and gabapentinoids to patients on opioid agonist therapy (OAT) are common and have pros and cons. The objectives of the current study are to define the dispensation rates of these potentially addictive drugs, and whether the number and the mean daily doses of dispensed OAT opioids and discontinuing OAT, are associated with being dispensed benzodiazepines, z-hypnotics and gabapentinoids among patients on OAT in Norway in the period 2013 to 2017.
Methods: Information about all dispensed opioids, benzodiazepines, z-hypnotics and gabapentinoids were recorded from the Norwegian Prescription Database (NorPD). A total of 10,371 OAT patients were included in the study period. The dispensation rates were defined as the number of patients who were dispensed at least one of the potentially addictive drugs divided among the number of patients who have dispensed an OAT opioid per calendar year. Mean daily doses were calculated, and for benzodiazepines and z-hypnotics, stated in diazepam equivalents. The association between dispensed potentially addictive drugs, and the number and the type of dispensed OAT opioids were calculated by using logistic regression models.
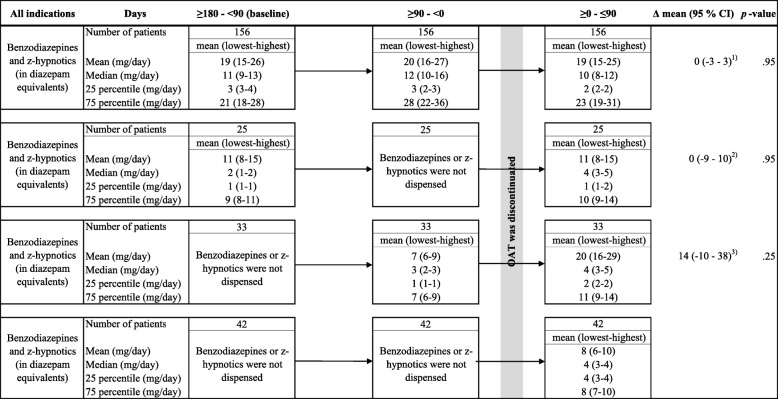
Results: Half of the OAT patients received at least one dispensation of a benzodiazepine or z-hypnotic, and 11% were dispensed at least a gabapentinoid in 2017. For dispensed benzodiazepines or z-hypnotics, the mean daily dose was reduced from 21 mg (95% confidence interval (CI): 20-23) diazepam equivalents in 2013 to 17 mg (95% CI: 16-17) in 2017. The mean daily dose of pregabalin increased from 365 mg (95% CI: 309-421) in 2013 to 386 mg (95% CI: 349-423) in 2017. Being dispensed a gabapentinoid (adjusted odds ratio (aOR) = 2.5, 95% CI: 2.1-3.0) or a non-OAT opioid (aOR = 3.0, 95% CI: 2.6-3.5) was associated with being dispensed a benzodiazepine or z-hypnotic. Discontinuing OAT did not affect the number of dispensations and the doses of potentially addictive drugs.
Conclusion: The dispensation rates of potentially addictive drugs are high in the OAT population. Treatment indications, as well as requirements for prescription authority, need to be debated and made explicit. Randomized controlled trials evaluating the benefits and risks of such co-prescription are required.
Keywords: Benzodiazepines; Drug prescriptions; Gabapentin; Opioid substitution treatment; Opioids; Pregabalin; Zolpidem; Zopiclone.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Abrahamsson T, Berge J, Ojehagen A, Hakansson A. Benzodiazepine, z-drug and pregabalin prescriptions and mortality among patients in opioid maintenance treatment-a nation-wide register-based open cohort study. Drug Alcohol Depend. 2017;174:58–64. doi: 10.1016/j.drugalcdep.2017.01.013. - DOI - PubMed
-
- Loxley W. Benozdiazepine use and harms among police detainees in Australia. Aust Inst Criminol. 2007;336:1.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
