

Immediate and long-term effects of BCI-based rehabilitation of the upper extremity after stroke: a systematic review and meta-analysis
- PMID: 32334608
- PMCID: PMC7183617
- DOI: 10.1186/s12984-020-00686-2
Immediate and long-term effects of BCI-based rehabilitation of the upper extremity after stroke: a systematic review and meta-analysis
Abstract
Background: A substantial number of clinical studies have demonstrated the functional recovery induced by the use of brain-computer interface (BCI) technology in patients after stroke. The objective of this review is to evaluate the effect sizes of clinical studies investigating the use of BCIs in restoring upper extremity function after stroke and the potentiating effect of transcranial direct current stimulation (tDCS) on BCI training for motor recovery.
Methods: The databases (PubMed, Medline, EMBASE, CINAHL, CENTRAL, PsycINFO, and PEDro) were systematically searched for eligible single-group or clinical controlled studies regarding the effects of BCIs in hemiparetic upper extremity recovery after stroke. Single-group studies were qualitatively described, but only controlled-trial studies were included in the meta-analysis. The PEDro scale was used to assess the methodological quality of the controlled studies. A meta-analysis of upper extremity function was performed by pooling the standardized mean difference (SMD). Subgroup meta-analyses regarding the use of external devices in combination with the application of BCIs were also carried out. We summarized the neural mechanism of the use of BCIs on stroke.
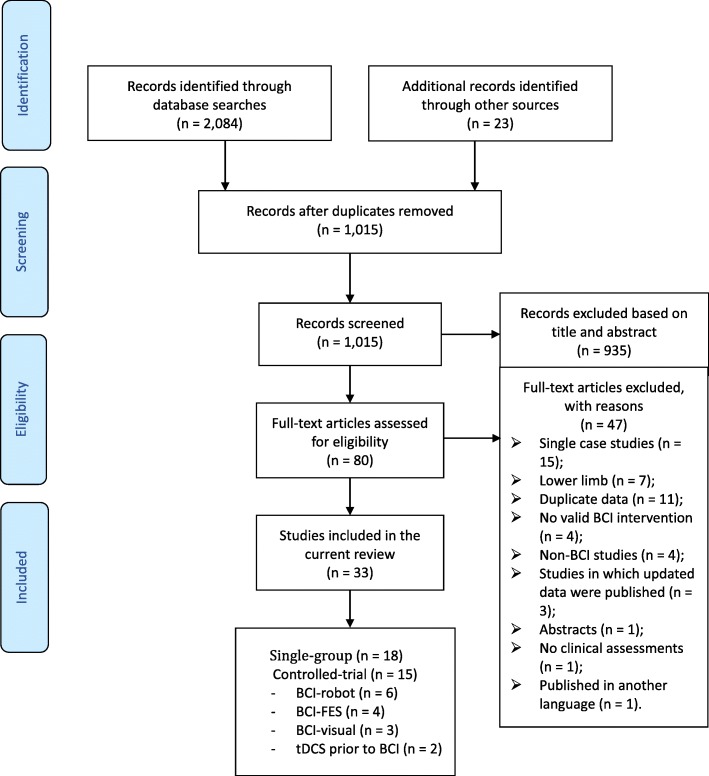
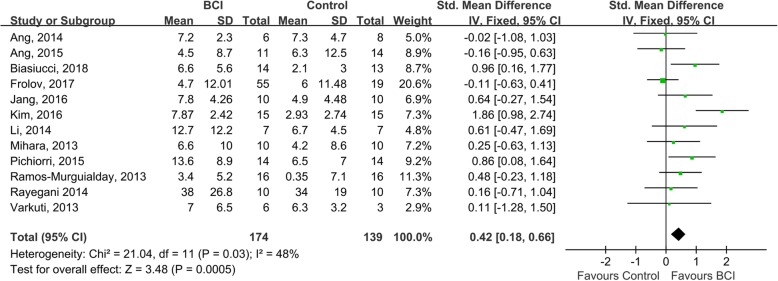
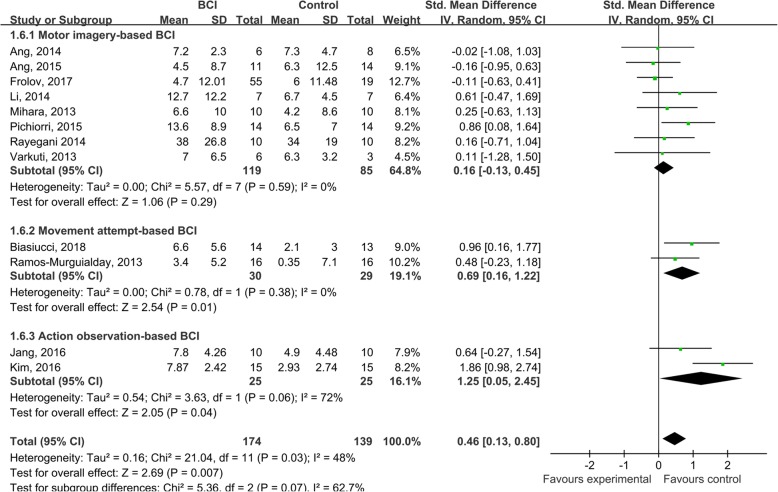
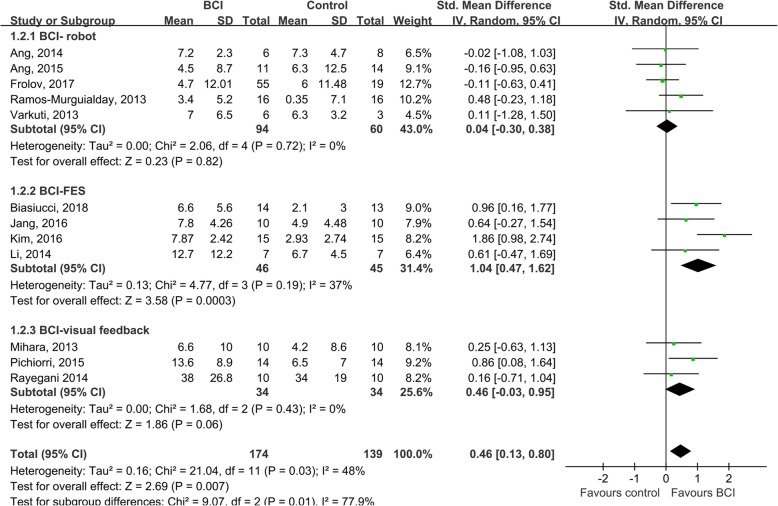
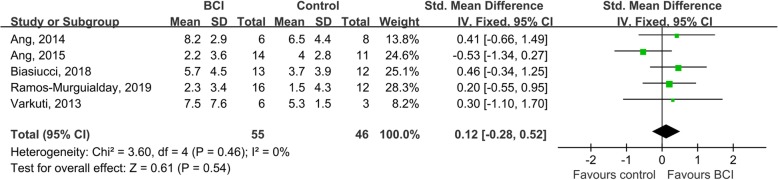
Results: A total of 1015 records were screened. Eighteen single-group studies and 15 controlled studies were included. The studies showed that BCIs seem to be safe for patients with stroke. The single-group studies consistently showed a trend that suggested BCIs were effective in improving upper extremity function. The meta-analysis (of 12 studies) showed a medium effect size favoring BCIs for improving upper extremity function after intervention (SMD = 0.42; 95% CI = 0.18-0.66; I2 = 48%; P < 0.001; fixed-effects model), while the long-term effect (five studies) was not significant (SMD = 0.12; 95% CI = - 0.28 - 0.52; I2 = 0%; P = 0.540; fixed-effects model). A subgroup meta-analysis indicated that using functional electrical stimulation as the external device in BCI training was more effective than using other devices (P = 0.010). Using movement attempts as the trigger task in BCI training appears to be more effective than using motor imagery (P = 0.070). The use of tDCS (two studies) could not further facilitate the effects of BCI training to restore upper extremity motor function (SMD = - 0.30; 95% CI = - 0.96 - 0.36; I2 = 0%; P = 0.370; fixed-effects model).
Conclusion: The use of BCIs has significant immediate effects on the improvement of hemiparetic upper extremity function in patients after stroke, but the limited number of studies does not support its long-term effects. BCIs combined with functional electrical stimulation may be a better combination for functional recovery than other kinds of neural feedback. The mechanism for functional recovery may be attributed to the activation of the ipsilesional premotor and sensorimotor cortical network.
Keywords: Brain-computer interface; Hemiparetic upper extremity function; Motor imagery; Movement attempt; Neural mechanism; Stroke.
Conflict of interest statement
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
