

Sex-specific clustering of metabolic risk factors and cancer risk: a longitudinal study in Iran
- PMID: 32334634
- PMCID: PMC7183600
- DOI: 10.1186/s13293-020-00296-6
Sex-specific clustering of metabolic risk factors and cancer risk: a longitudinal study in Iran
Abstract
Background: Cancer is a major cause of death in low- and middle-income countries. A large number of studies have shown that some of the metabolic risk factors (MRFs) tend to cluster in individuals. We examined the synergistic effects of multiple MRFs and cancer risk among Iranian adults.
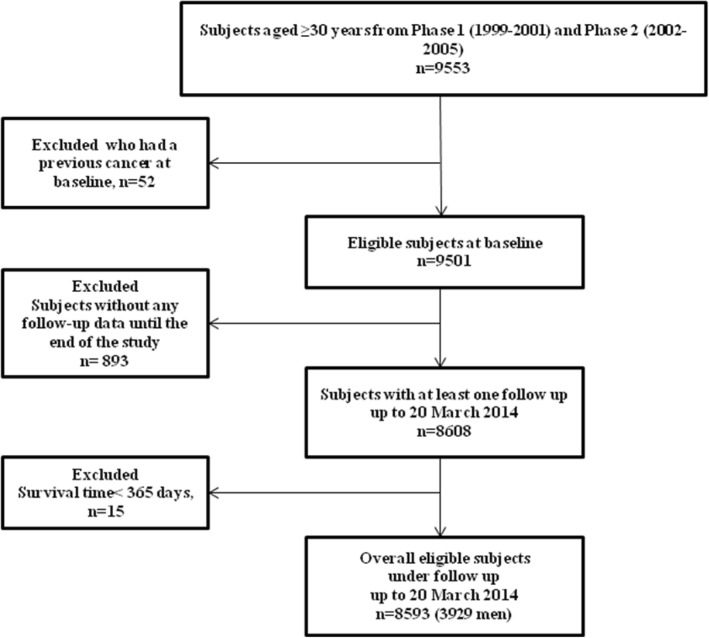
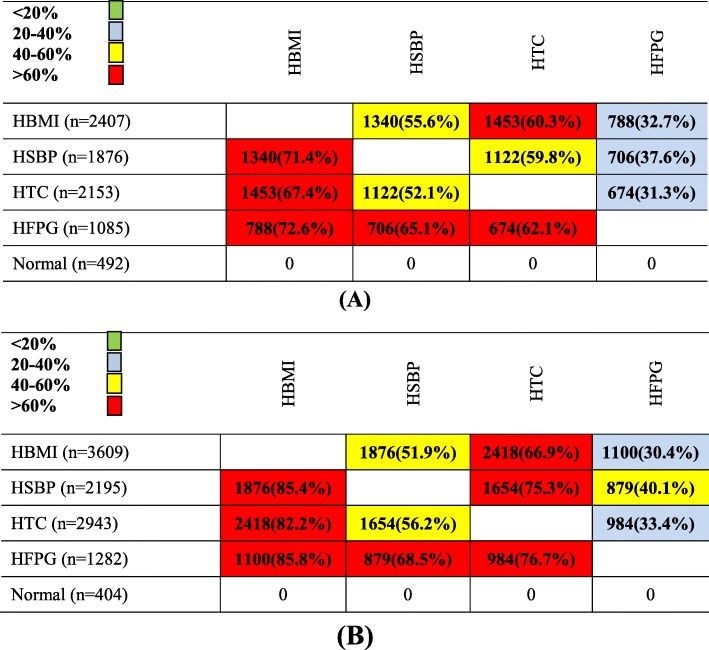
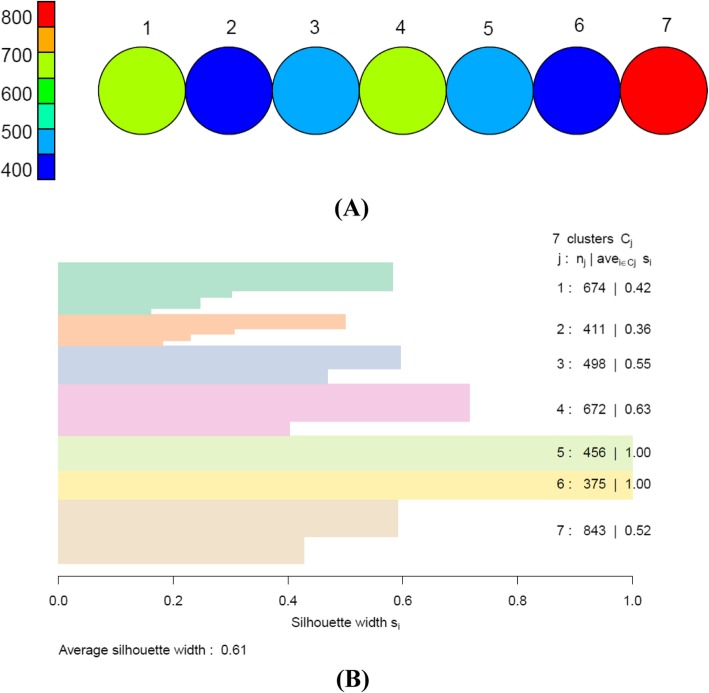
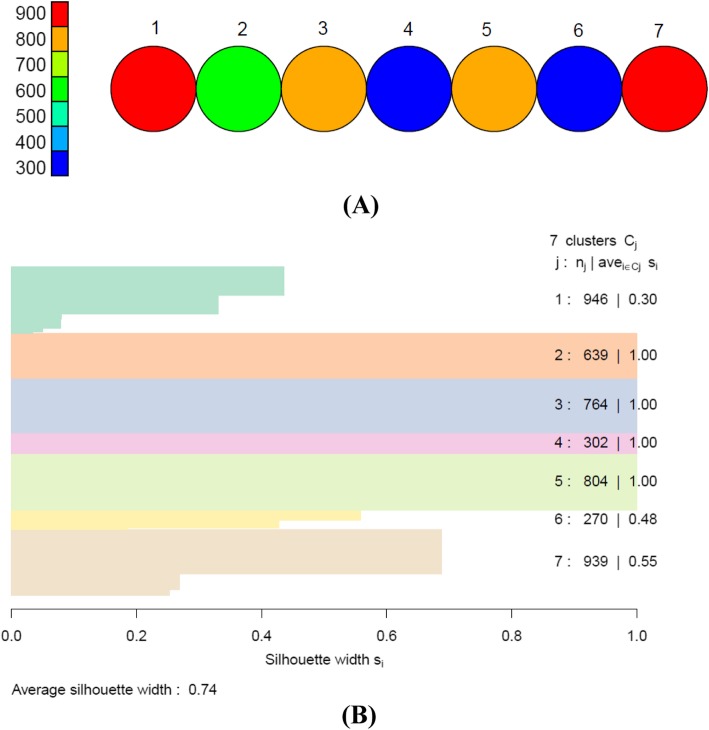
Methods: Among 8593 (3929 men) participants aged ≥ 30 years, the self-organizing map (SOM) was applied to clustering of four MRFs including high fasting plasma glucose (HFPG), high total cholesterol (HTC), high systolic blood pressure (HSBP), and high body mass index (HBMI). The Cox proportional hazards model was used to investigate the association between clusters with cancer incidence during a median of 14.0 years of follow-up.
Results: During the study period, 265 new cases of cancer were identified among participants at risk. The incidence density rate was 2.5 per 1000 person years in total population. About 32 and 40% of men and women, respectively, had three or four MRFs. We identified seven clusters of MRFs in both men and women. In both genders, MRFs were clustered in those with older age. Further, inverse associations were found between current smoking in men, and education level and passive smoking in women and clustering of MRFs. In men, a cluster with 100% HSBP and HBMI had the highest risk for overall cancer. While, among women, a cluster with 100% HFPG and 93% HBMI yielded the highest risk for cancer. The risk was decreased when HBMI accompanied by HTC.
Conclusions: Clustering patterns may reflect underlying link between MRFs and cancer and could potentially facilitate tailored health promotion interventions.
Keywords: Cancer; Cluster; Metabolic; Risk factor.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Gelband H, Jha P, Sankaranarayanan R, Horton S, editors. Cancer: Disease Control Priorities, 3rd edn. Washington (DC): The International Bank for Reconstruction and Development/The World Bank; 2015. - PubMed
-
- Atun R, Knaul FM, Gospodarowicz M. Networks in global cancer-potential synergies and opportunities. Lancet Glob Health. 2018;6:S21–S22. doi: 10.1016/S2214-109X(18)30093-7. - DOI
-
- Shabestari AN, Moghaddam SS, Sharifi F, Fadayevatan R, Nabavizadeh F, Delavari A, et al. The most prevalent causes of deaths, DALYs, and geriatric syndromes in Iranian elderly people between 1990 and 2010: findings from the Global Burden of Disease study 2010. Arch Iran Med. 2015;18(8):462–479. - PubMed
-
- Gakidou E, Afshin A, Abajobir AA, Abate KH, Abbafati C, Abbas KM, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345–1422. doi: 10.1016/S0140-6736(17)32366-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
