

Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis
- PMID: 32335169
- PMCID: PMC7177098
- DOI: 10.1016/j.jinf.2020.04.021
Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis
Abstract
Background: An epidemic of Coronavirus Disease 2019 (COVID-19) began in December 2019 and triggered a Public Health Emergency of International Concern (PHEIC). We aimed to find risk factors for the progression of COVID-19 to help reducing the risk of critical illness and death for clinical help.
Methods: The data of COVID-19 patients until March 20, 2020 were retrieved from four databases. We statistically analyzed the risk factors of critical/mortal and non-critical COVID-19 patients with meta-analysis.
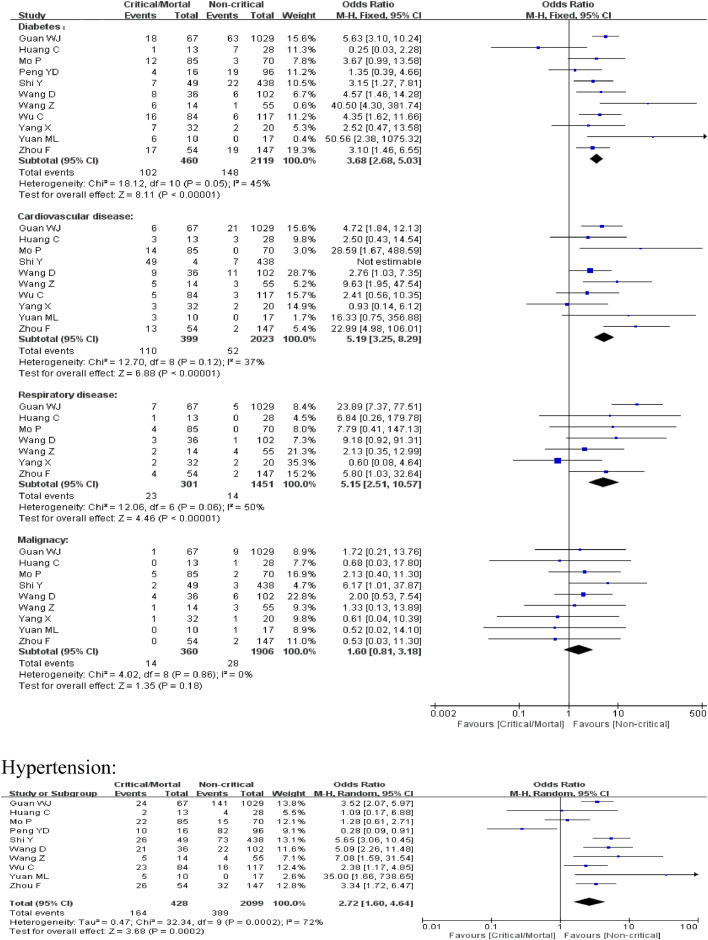
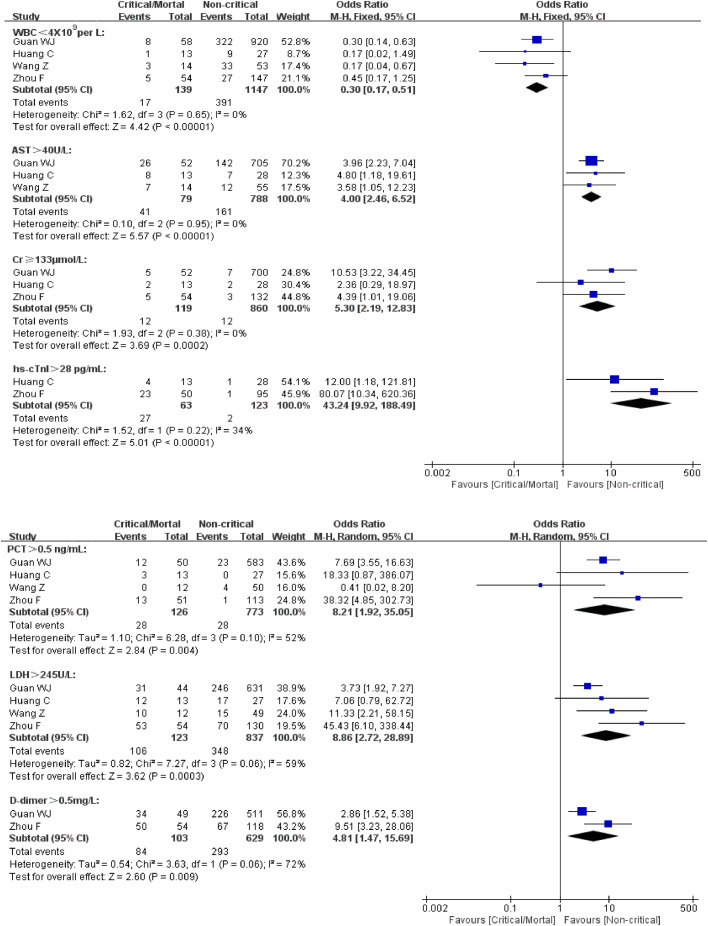
Results: Thirteen studies were included in Meta-analysis, including a total number of 3027 patients with SARS-CoV-2 infection. Male, older than 65, and smoking were risk factors for disease progression in patients with COVID-19 (male: OR = 1.76, 95% CI (1.41, 2.18), P < 0.00001; age over 65 years old: OR =6.06, 95% CI(3.98, 9.22), P < 0.00001; current smoking: OR =2.51, 95% CI(1.39, 3.32), P = 0.0006). The proportion of underlying diseases such as hypertension, diabetes, cardiovascular disease, and respiratory disease were statistically significant higher in critical/mortal patients compared to the non-critical patients (diabetes: OR=3.68, 95% CI (2.68, 5.03), P < 0.00001; hypertension: OR = 2.72, 95% CI (1.60,4.64), P = 0.0002; cardiovascular disease: OR = 5.19, 95% CI(3.25, 8.29), P < 0.00001; respiratory disease: OR = 5.15, 95% CI(2.51, 10.57), P < 0.00001). Clinical manifestations such as fever, shortness of breath or dyspnea were associated with the progression of disease [fever: 0R = 0.56, 95% CI (0.38, 0.82), P = 0.003;shortness of breath or dyspnea: 0R=4.16, 95% CI (3.13, 5.53), P < 0.00001]. Laboratory examination such as aspartate amino transferase(AST) > 40U/L, creatinine(Cr) ≥ 133mol/L, hypersensitive cardiac troponin I(hs-cTnI) > 28pg/mL, procalcitonin(PCT) > 0.5ng/mL, lactatede hydrogenase(LDH) > 245U/L, and D-dimer > 0.5mg/L predicted the deterioration of disease while white blood cells(WBC)<4 × 109/L meant a better clinical status[AST > 40U/L:OR=4.00, 95% CI (2.46, 6.52), P < 0.00001; Cr ≥ 133μmol/L: OR = 5.30, 95% CI (2.19, 12.83), P = 0.0002; hs-cTnI > 28 pg/mL: OR = 43.24, 95% CI (9.92, 188.49), P < 0.00001; PCT > 0.5 ng/mL: OR = 43.24, 95% CI (9.92, 188.49), P < 0.00001;LDH > 245U/L: OR = 43.24, 95% CI (9.92, 188.49), P < 0.00001; D-dimer > 0.5mg/L: OR = 43.24, 95% CI (9.92, 188.49), P < 0.00001; WBC < 4 × 109/L: OR = 0.30, 95% CI (0.17, 0.51), P < 0.00001].
Conclusion: Male, aged over 65, smoking patients might face a greater risk of developing into the critical or mortal condition and the comorbidities such as hypertension, diabetes, cardiovascular disease, and respiratory diseases could also greatly affect the prognosis of the COVID-19. Clinical manifestation such as fever, shortness of breath or dyspnea and laboratory examination such as WBC, AST, Cr, PCT, LDH, hs-cTnI and D-dimer could imply the progression of COVID-19.
Keywords: COVID-19; Clinical manifestation; Comorbidity; Laboratory examination; Risk factor.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures


Comment in
-
Acute kidney injury in hospitalized patients with coronavirus disease 2019 (COVID-19): A meta-analysis.J Infect. 2020 Oct;81(4):647-679. doi: 10.1016/j.jinf.2020.05.009. Epub 2020 May 8. J Infect. 2020. PMID: 32389782 Free PMC article. No abstract available.
-
Clinical course of severe and critically ill patients with coronavirus disease 2019 (COVID-19): A comparative study.J Infect. 2020 Aug;81(2):e82-e84. doi: 10.1016/j.jinf.2020.05.021. Epub 2020 May 13. J Infect. 2020. PMID: 32405109 Free PMC article. No abstract available.
-
Clinical and conceptual comments on "Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis".J Infect. 2020 Oct;81(4):647-679. doi: 10.1016/j.jinf.2020.05.011. Epub 2020 May 11. J Infect. 2020. PMID: 32407756 Free PMC article. No abstract available.
-
Age but not sex may explain the negative effect of arterial hypertension and diabetes on COVID-19 prognosis.J Infect. 2020 Oct;81(4):647-679. doi: 10.1016/j.jinf.2020.05.010. Epub 2020 May 11. J Infect. 2020. PMID: 32407757 Free PMC article. No abstract available.
-
Short-term outcomes in individuals aged 75 or older with severe coronavirus disease (COVID-19): First observations from an infectious diseases unit in Southern Italy.J Infect. 2020 Aug;81(2):e86-e88. doi: 10.1016/j.jinf.2020.05.024. Epub 2020 May 14. J Infect. 2020. PMID: 32417315 Free PMC article. No abstract available.
-
Dyspnea rather than fever is a risk factor for predicting mortality in patients with COVID-19.J Infect. 2020 Oct;81(4):647-679. doi: 10.1016/j.jinf.2020.05.013. Epub 2020 May 15. J Infect. 2020. PMID: 32417316 Free PMC article. No abstract available.
-
Which cancer type has the highest risk of COVID-19 infection?J Infect. 2020 Oct;81(4):647-679. doi: 10.1016/j.jinf.2020.05.028. Epub 2020 May 19. J Infect. 2020. PMID: 32442454 Free PMC article. No abstract available.
-
Cardiovascular disease as a risk factor of disease progression in COVID-19: The corrected effect size and forest plot.J Infect. 2020 Nov;81(5):816-846. doi: 10.1016/j.jinf.2020.05.038. Epub 2020 May 27. J Infect. 2020. PMID: 32473231 Free PMC article. No abstract available.
-
Drinking no-links to the severity of COVID-19: a systematic review and meta-analysis.J Infect. 2020 Aug;81(2):e126-e127. doi: 10.1016/j.jinf.2020.05.042. Epub 2020 May 28. J Infect. 2020. PMID: 32474047 Free PMC article. No abstract available.
-
The association of hypertension with the severity and mortality of COVID-19 patients: Evidence based on adjusted effect estimates.J Infect. 2020 Sep;81(3):e44-e47. doi: 10.1016/j.jinf.2020.06.060. Epub 2020 Jun 25. J Infect. 2020. PMID: 32593655 Free PMC article. No abstract available.
-
The potential indicators for pulmonary fibrosis in survivors of severe COVID-19.J Infect. 2021 Feb;82(2):e5-e7. doi: 10.1016/j.jinf.2020.09.027. Epub 2020 Sep 28. J Infect. 2021. PMID: 32998036 Free PMC article. No abstract available.
-
Is creatinine an independent risk factor for predicting adverse outcomes in COVID-19 patients?Transpl Infect Dis. 2021 Apr;23(2):e13539. doi: 10.1111/tid.13539. Epub 2020 Dec 12. Transpl Infect Dis. 2021. PMID: 33254281 Free PMC article. No abstract available.
References
-
- Lai C C, Wang C Y, Wang Y H. Global epidemiology of coronavirus disease 2019: disease incidence, daily cumulative index, mortality, and their association with country healthcare resources and economic status.[J] Int J Antimicrob Agents. 2020 doi: 10.1016/j.ijantimicag.2020.105946. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
