

Kidney Histopathology and Prediction of Kidney Failure: A Retrospective Cohort Study
- PMID: 32336487
- PMCID: PMC7483298
- DOI: 10.1053/j.ajkd.2019.12.014
Kidney Histopathology and Prediction of Kidney Failure: A Retrospective Cohort Study
Abstract
Rationale & objective: The use of kidney histopathology for predicting kidney failure is not established. We hypothesized that the use of histopathologic features of kidney biopsy specimens would improve prediction of clinical outcomes made using demographic and clinical variables alone.
Study design: Retrospective cohort study and development of a clinical prediction model.
Setting & participants: All 2,720 individuals from the Biopsy Biobank Cohort of Indiana who underwent kidney biopsy between 2002 and 2015 and had at least 2 years of follow-up.
New predictors & established predictors: Demographic variables, comorbid conditions, baseline clinical characteristics, and histopathologic features.
Outcomes: Time to kidney failure, defined as sustained estimated glomerular filtration rate ≤ 10mL/min/1.73m2.
Analytical approach: Multivariable Cox regression model with internal validation by bootstrapping. Models including clinical and demographic variables were fit with the addition of histopathologic features. To assess the impact of adding a histopathology variable, the amount of variance explained (r2) and the C index were calculated. The impact on prediction was assessed by calculating the net reclassification index for each histopathologic variable and for all combined.
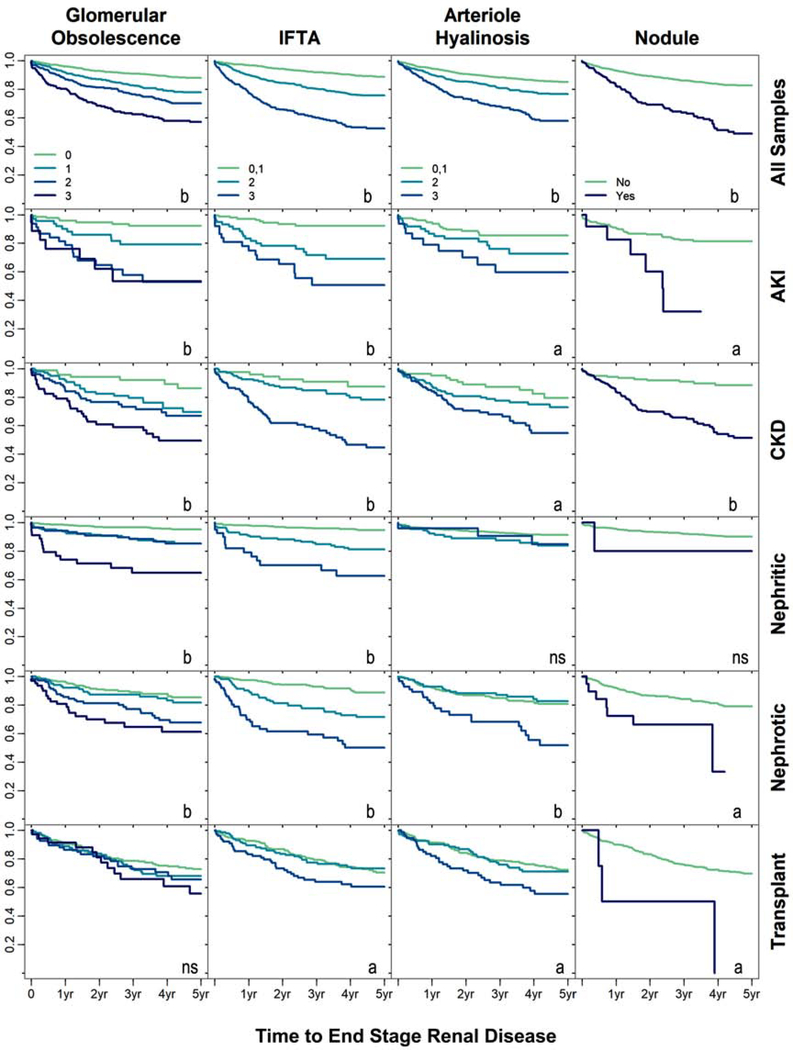
Results: Median follow-up was 3.1 years. Within 5 years of biopsy, 411 (15.1%) patients developed kidney failure. Multivariable analyses including demographic and clinical variables revealed that severe glomerular obsolescence (adjusted HR, 2.03; 95% CI, 1.51-2.03), severe interstitial fibrosis and tubular atrophy (adjusted HR, 1.99; 95% CI, 1.52-2.59), and severe arteriolar hyalinosis (adjusted HR, 1.53; 95% CI, 1.14-2.05) were independently associated with the primary outcome. The addition of all histopathologic variables to the clinical model yielded a net reclassification index for kidney failure of 5.1% (P < 0.001) with a full model C statistic of 0.915. Analyses addressing the competing risk for death, optimism, or shrinkage did not significantly change the results.
Limitations: Selection bias from the use of clinically indicated biopsies and exclusion of patients with less than 2 years of follow-up, as well as reliance on surrogate indicators of kidney failure onset.
Conclusions: A model incorporating histopathologic features from kidney biopsy specimens improved prediction of kidney failure and may be valuable clinically. Future studies will be needed to understand whether even more detailed characterization of kidney tissue may further improve prognostication about the future trajectory of estimated glomerular filtration rate.
Keywords: Kidney biopsy; clinical prognostication; disease progression; eGFR trajectory; end-stage renal disease (ESRD); estimated glomerular filtration rate (eGFR); glomerular obsolescence; histopathology; interstitial fibrosis and tubular atrophy (IFTA); prognostic prediction model; renal failure.
Copyright © 2020 National Kidney Foundation, Inc. All rights reserved.
Figures
References
-
- Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure. Jama. 2011;305(15): 1553–1559. - PubMed
-
- Chronic Kidney Disease Prognosis C. Grams ME, Sang Y, Ballew SH, et al., for the Chronic Kidney Disease Prognosis Consortium. Predicting timing of clinical outcomes in patients with chronic kidney disease and severely decreased glomerular filtration rate. Kidney Int. 2018;93:1442–1451. Kidney Int. 2018;94(5): 1025–1026. - PMC - PubMed
-
- Covic A, Schiller A, Volovat C, et al. Epidemiology of renal disease in Romania: a 10 year review of two regional renal biopsy databases. Nephrol Dial Transplant. 2006;21(2): 419–424. - PubMed
-
- Rychlik I, Jancova E, Tesar V, et al. The Czech registry of renal biopsies. Occurrence of renal diseases in the years 1994–2000. Nephrol Dial Transplant. 2004;19(12): 3040–3049. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
