

Inflammatory diseases of the nasal cavities and paranasal sinuses
- PMID: 32336992
- PMCID: PMC7172334
- DOI: 10.1016/j.mpdhp.2010.03.008
Inflammatory diseases of the nasal cavities and paranasal sinuses
Abstract
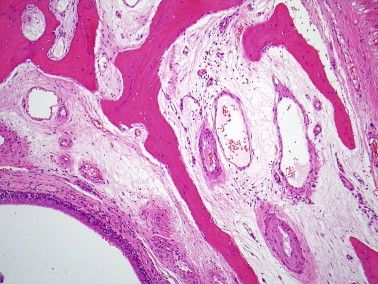
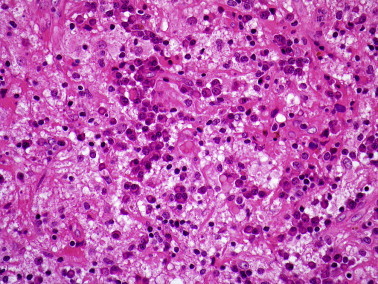
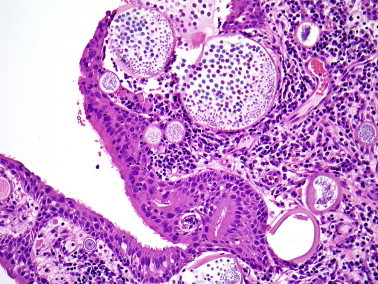
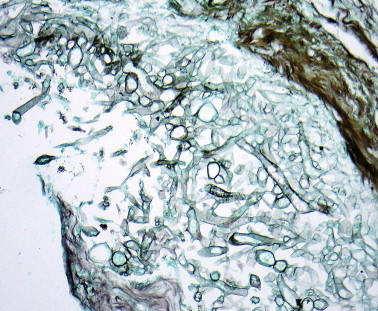
Inflammatory diseases of the nose and paranasal sinus are commonly encountered in diagnostic histopathology. This review describes the possible manifestations of the common diseases as well as highlighting some of the uncommon causes of sinonasal inflammation which may have importance for treatment and prognosis. The diagnosis of fungal sinusitis is primarily histological. It is important to distinguish between invasive and non-invasive fungal sinusitis, the latter including allergic fungal sinusitis characterized by 'allergic mucin' and scanty fungal hyphae. Nasal eosinophilia is a feature of both allergic and non-allergic rhinosinusitis and a wide range of secondary changes in inflammatory polyps may lead to diagnostic confusion. Nasal biopsies are often taken from perforations or inflammatory masses to confirm or exclude granulomatous diseases. There is a broad differential diagnosis for granulomatous sinonasal disease and pathologists should appreciate the diagnostic histological and clinical features of these conditions.
Keywords: chronic inflammation; diagnosis; fungal diseases; granulomatous inflammation; nose and paranasal sinuses; pathology.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures














References
-
- Kim Y.M., Kim A.Y., Park Y.H., Kim D.H., Rha K.S. Eight cases of nasal tuberculosis. Otolaryngol Head Neck Surg. 2007;137:500–504. - PubMed
-
- Melo Naves M., Gomes Patrocinio L., Patrocinio J.A. Contribution of nasal biopsy to leprosy diagnosis. Am J Rhinol Allergy. 2009;23:177–180. - PubMed
-
- de Pontual L., Ovetchkine P., Rodriguez D. Rhinoscleroma: a French national retrospective study of epidemiological and clinical features. Clin Infect Dis. 2008;47:1396–1402. - PubMed
-
- Hart C.A., Rao S.K. Rhinoscleroma. J Med Microbiol. 2000;49:395–396. - PubMed
LinkOut - more resources
Full Text Sources