

Toronto Workshop on Late Recurrence in Estrogen Receptor-Positive Breast Cancer: Part 2: Approaches to Predict and Identify Late Recurrence, Research Directions
- PMID: 32337478
- PMCID: PMC7050024
- DOI: 10.1093/jncics/pkz049
Toronto Workshop on Late Recurrence in Estrogen Receptor-Positive Breast Cancer: Part 2: Approaches to Predict and Identify Late Recurrence, Research Directions
Abstract
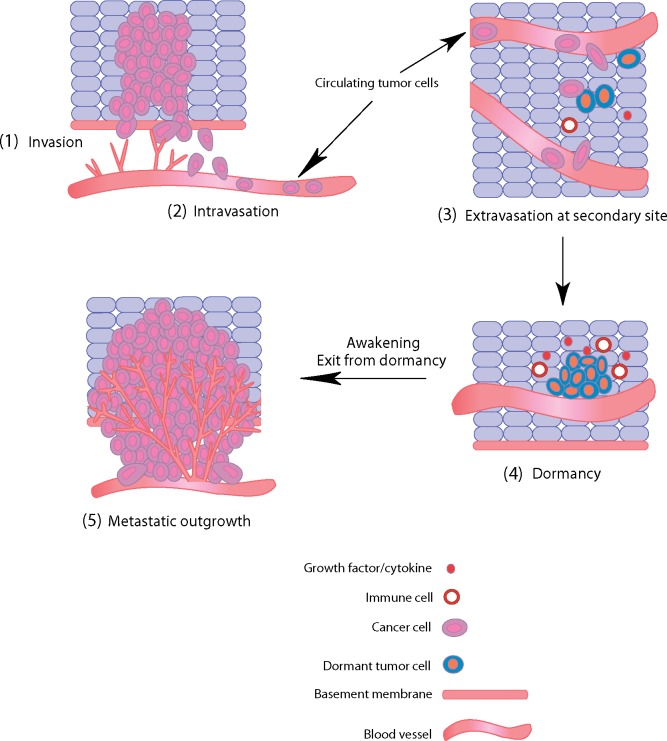
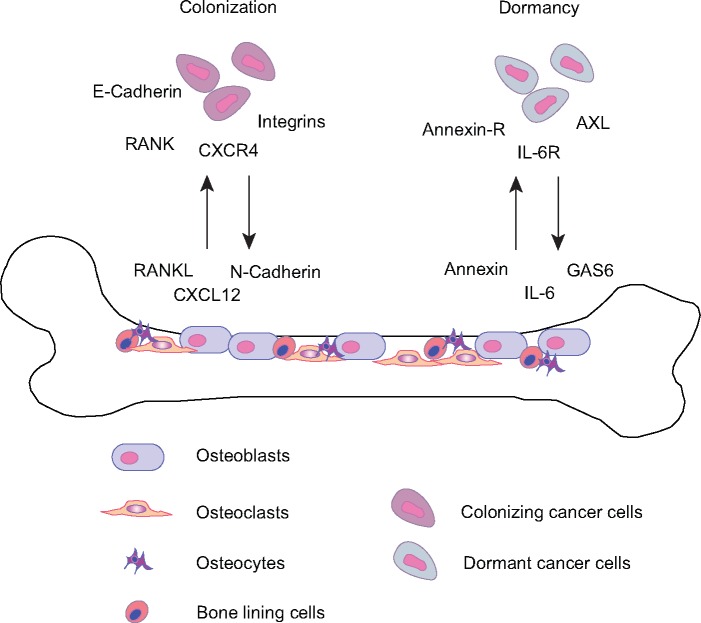
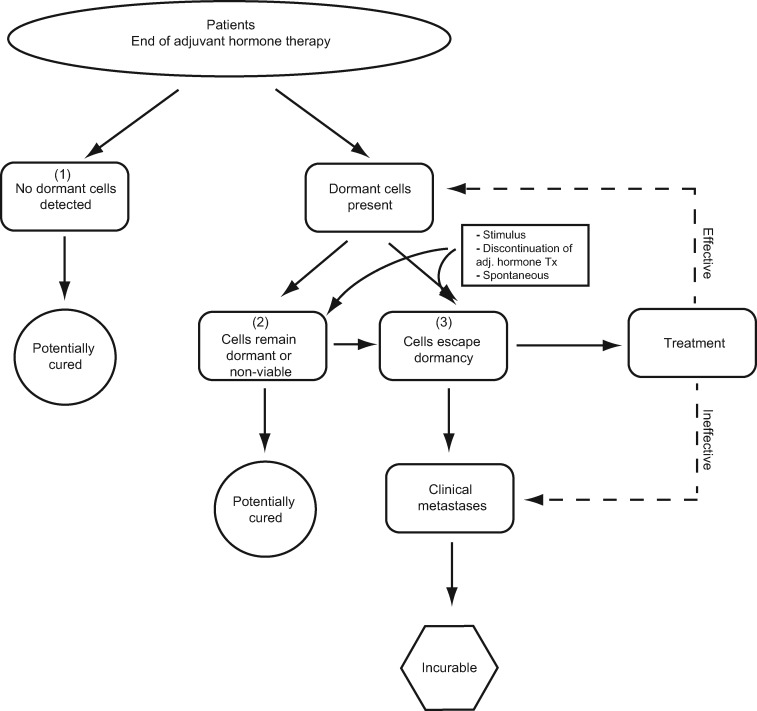
Late disease recurrence (more than 5 years after initial diagnosis) represents a clinical challenge in the treatment and management of estrogen receptor-positive breast cancer (BC). An international workshop was convened in Toronto, Canada, in February 2018 to review the current understanding of late recurrence and to identify critical issues that require future study. The underlying biological causes of late recurrence are complex, with the processes governing cancer cell dormancy, including immunosurveillance, cell proliferation, angiogenesis, and cellular stemness, being integral to disease progression. These critical processes are described herein as well as their role in influencing risk of recurrence. Moreover, observational and interventional clinical trials are proposed, with a focus on methods to identify patients at risk of recurrence and possible strategies to combat this in patients with estrogen receptor-positive BC. Because the problem of late BC recurrence of great importance, recent advances in disease detection and patient monitoring should be incorporated into novel clinical trials to evaluate approaches to enhance patient management. Indeed, future research on these issues is planned and will offer new options for effective late recurrence treatment and prevention strategies.
© The Author(s) 2019. Published by Oxford University Press.
Figures
References
-
- Hensel JA, Flaig TW, Theodorescu D.. Clinical opportunities and challenges in targeting tumour dormancy. Nat Rev Clin Oncol. 2013;10(1):41–51. - PubMed
-
- Dittmer J. Mechanisms governing metastatic dormancy in breast cancer. Semin Cancer Biol. 2017;44:72–82. - PubMed
-
- Trumpp A, Essers M, Wilson A.. Awakening dormant haematopoietic stem cells. Nat Rev Immunol. 2010;10(3):201–209. - PubMed
LinkOut - more resources
Full Text Sources