

Guillain-Barré syndrome related to Zika virus infection: A systematic review and meta-analysis of the clinical and electrophysiological phenotype
- PMID: 32339199
- PMCID: PMC7205322
- DOI: 10.1371/journal.pntd.0008264
Guillain-Barré syndrome related to Zika virus infection: A systematic review and meta-analysis of the clinical and electrophysiological phenotype
Abstract
Background: The Zika virus (ZIKV) has been associated with Guillain-Barré syndrome (GBS) in epidemiological studies. Whether ZIKV-associated GBS is related to a specific clinical or electrophysiological phenotype has not been established. To this end, we performed a systematic review and meta-analysis of all published studies on ZIKV-related GBS.
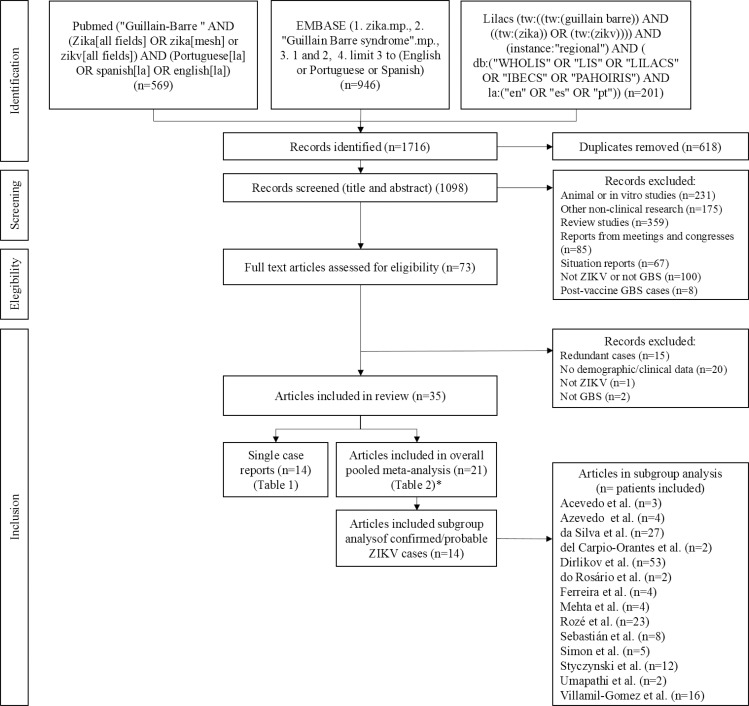
Methods: We searched Pubmed, EMBASE and LILACS, and included all papers, reports or bulletins with full text in English, Spanish or Portuguese, reporting original data of patients with GBS and a suspected, probable or confirmed recent ZIKV infection. Data were extracted according to a predefined protocol, and pooled proportions were calculated.
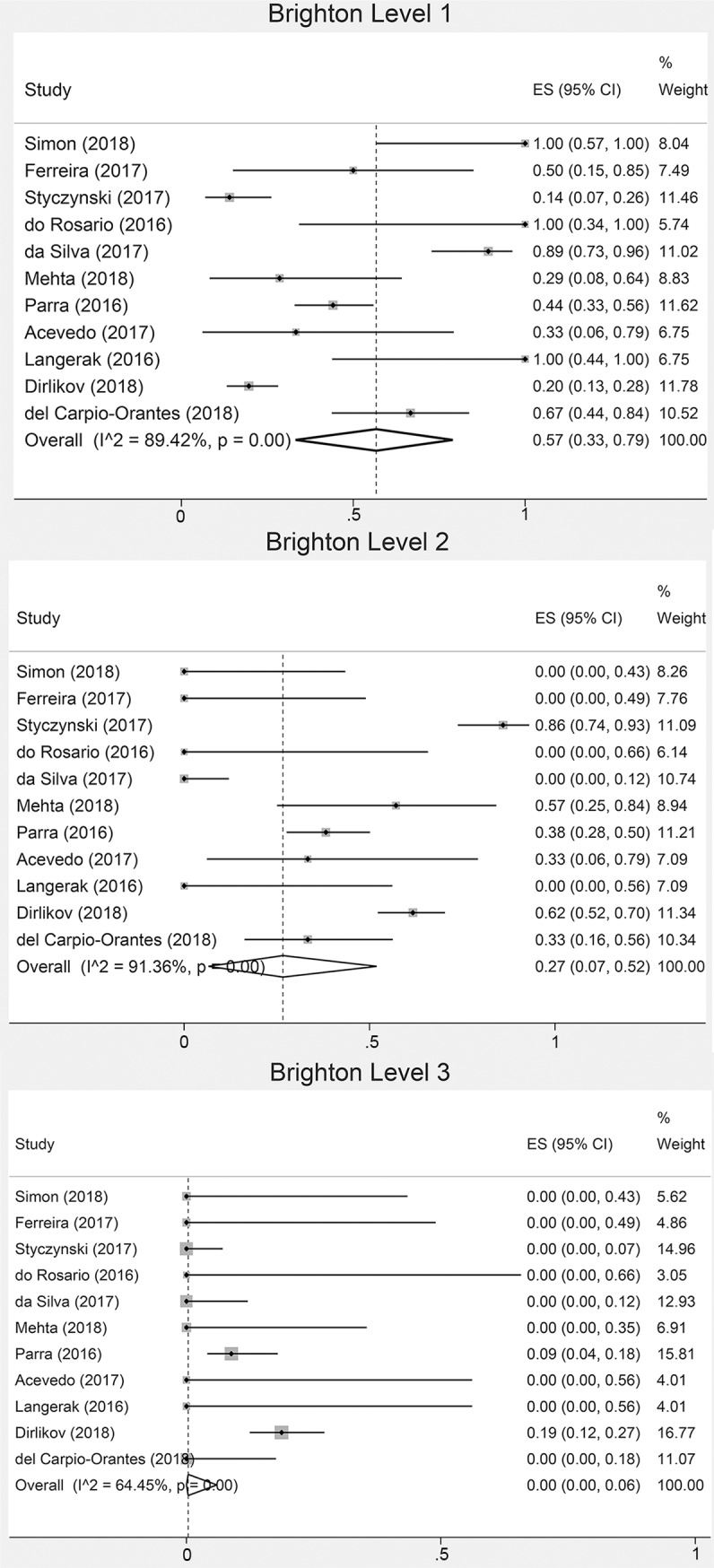
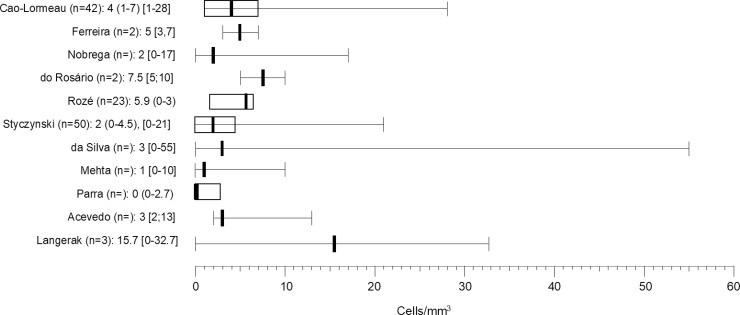
Results: Thirty-five studies were included (13 single case reports and 22 case series, case-control or cohort studies), reporting on a total of 601 GBS patients with a suspected, probable or confirmed ZIKV infection. Data from 21 studies and 587 cases were available to be summarized. ZIKV infection was confirmed in 21%, probable in 22% and suspected in 57% of cases. ZIKV PCR was positive in 30% (95%CI 15-47) of tested patients. The most common clinical features were: limb weakness 97% (95%CI 93-99), diminished/absent reflexes 96% (95%CI 88-100), sensory symptoms 82% (95%CI 76-88), and facial palsy 51% (95%CI 44-58). Median time between infectious and neurological symptoms was 5-12 days. Most cases had a demyelinating electrophysiological subtype and half of cases were admitted to the Intensive Care Unit (ICU). Heterogeneity between studies was moderate to substantial for most variables.
Conclusions: The clinical phenotype of GBS associated with ZIKV infection reported in literature is generally a sensorimotor demyelinating GBS with frequent facial palsy and a severe disease course often necessitating ICU admittance. Time between infectious and neurological symptoms and negative PCR in most cases suggests a post-infectious disease mechanism. Heterogeneity between studies was considerable and results may be subject to reporting bias. This study was registered on the international Prospective Register of Systematic Reviews (CRD42018081959).
Conflict of interest statement
SEL, CCBS, MLBF, JLB, SC and MFPMA declare no competing interests. BCJ has received funding from Annexon Biosciences, Baxter, CSL Behring, Hansa Biopharma and Grifols.
Figures

References
-
- World Health Organization. Zika situation report 5 February 2016. World Health Organization; 2016:Available from: https://www.who.int/emergencies/zika-virus/situation-report/5-february-2....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
