

Simultaneous Metabolic and Perfusion Imaging Using Hyperpolarized 13C MRI Can Evaluate Early and Dose-Dependent Response to Radiation Therapy in a Prostate Cancer Mouse Model
- PMID: 32339646
- PMCID: PMC7381368
- DOI: 10.1016/j.ijrobp.2020.04.022
Simultaneous Metabolic and Perfusion Imaging Using Hyperpolarized 13C MRI Can Evaluate Early and Dose-Dependent Response to Radiation Therapy in a Prostate Cancer Mouse Model
Abstract
Purpose: To investigate use of a novel imaging approach, hyperpolarized (HP) 13C magnetic resonance imaging (MRI) for simultaneous metabolism and perfusion assessment, to evaluate early and dose-dependent response to radiation therapy (RT) in a prostate cancer mouse model.
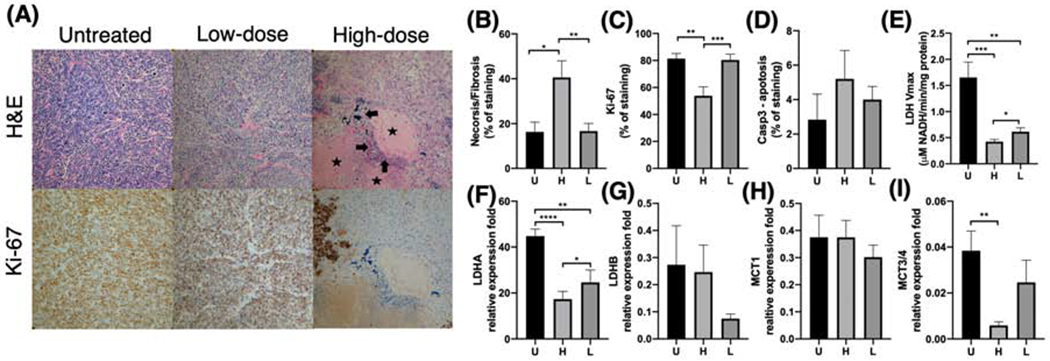
Methods and materials: Transgenic Adenocarcinoma of Mouse Prostate (TRAMP) mice (n = 18) underwent single-fraction RT (4-14 Gy steep dose across the tumor) and were imaged serially at pre-RT baseline and 1, 4, and 7 days after RT using HP 13C MRI with combined [1-13C]pyruvate (metabolic active agent) and [13C]urea (perfusion agent), coupled with conventional multiparametric 1H MRI including T2-weighted, dynamic contrast-enhanced, and diffusion-weighted imaging. Tumor tissues were collected 4 and 7 days after RT for biological correlative studies.
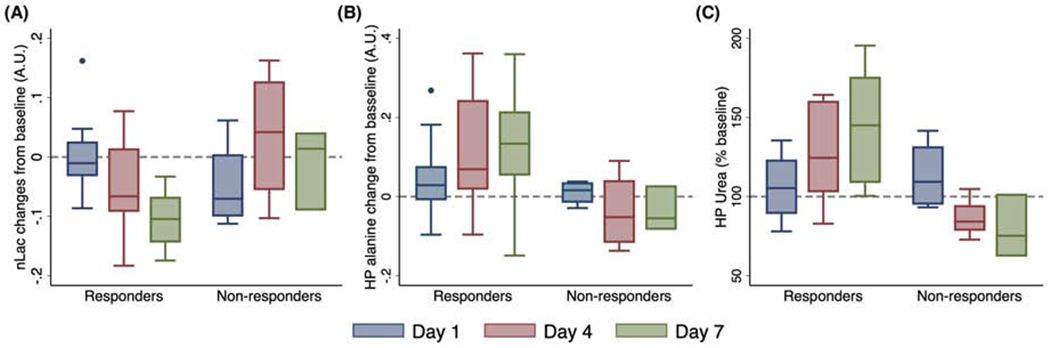
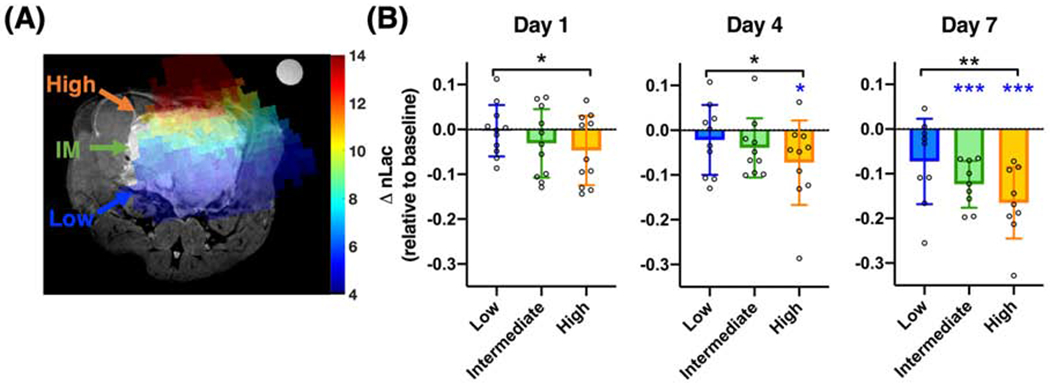
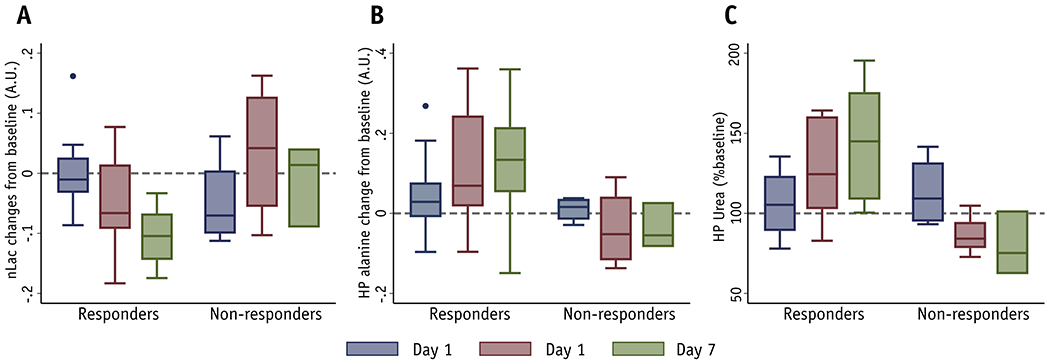
Results: We found a significant decrease in HP pyruvate-to-lactate conversion in tumors responding to RT, with concomitant significant increases in HP pyruvate-to-alanine conversion and HP urea signal; the opposite changes were observed in tumors resistant to RT. Moreover, HP lactate change was dependent on radiation dose; tumor regions treated with higher radiation doses (10-14 Gy) exhibited a greater decrease in HP lactate signal than low-dose regions (4-7 Gy) as early as 1 day post-RT, consistent with lactate dehydrogenase enzyme activity and expression data. We also found that HP [13C]urea MRI provided assessments of tumor perfusion similar to those provided by 1H dynamic contrast-enhanced MRI in this animal model. However, apparent diffusion coefficien , a conventional 1H MRI functional biomarker, did not exhibit statistically significant changes within 7 days after RT.
Conclusion: These results demonstrate the ability of HP 13C MRI to monitor radiation-induced physiologic changes in a timely and dose-dependent manner, providing the basic science premise for further clinical investigation and translation.
Copyright © 2020 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Sanda MG, Cadeddu JA, Kirkby E, et al. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. part I: risk stratification, shared decision making, and care options. J. Urol. 2018;199:683–690. - PubMed
-
- Chin J, Rumble RB, Kollmeier M, et al. Brachytherapy for patients with prostate cancer: american society of clinical oncology/cancer care ontario joint guideline update. J. Clin. Oncol. 2017;35: 1737–1743. - PubMed
-
- Roach M, Hanks G, Thames H, et al. Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006;65:965–974. - PubMed
-
- Cox JD, Gallagher MJ, Hammond EH, et al. Consensus statements on radiation therapy of prostate cancer: guidelines for prostate re-biopsy after radiation and for radiation therapy with rising prostate-specific antigen levels after radical prostatectomy. American Society for Therapeutic Radiology and Oncology Consensus Panel. J. Clin. Oncol. 1999; 17:1155. - PubMed
-
- Jalloh M, Leapman MS, Cowan JE, et al. Patterns of Local Failure following Radiation Therapy for Prostate Cancer. J. Urol. 2015;194:977–982. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
