

Analysis of the Healthcare MERS-CoV Outbreak in King Abdulaziz Medical Center, Riyadh, Saudi Arabia, June-August 2015 Using a SEIR Ward Transmission Model
- PMID: 32340361
- PMCID: PMC7215950
- DOI: 10.3390/ijerph17082936
Analysis of the Healthcare MERS-CoV Outbreak in King Abdulaziz Medical Center, Riyadh, Saudi Arabia, June-August 2015 Using a SEIR Ward Transmission Model
Abstract
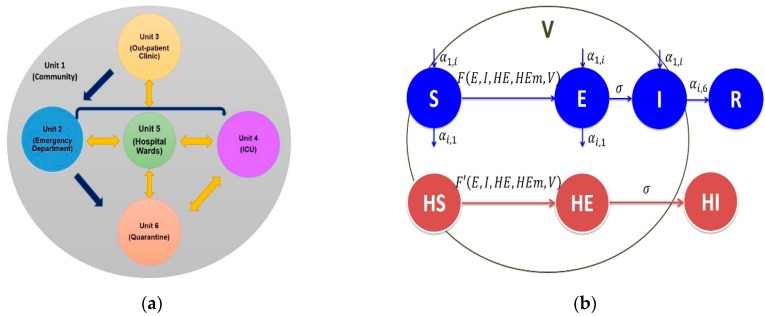
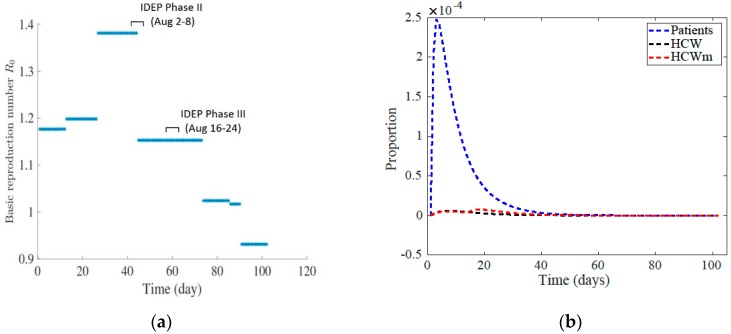
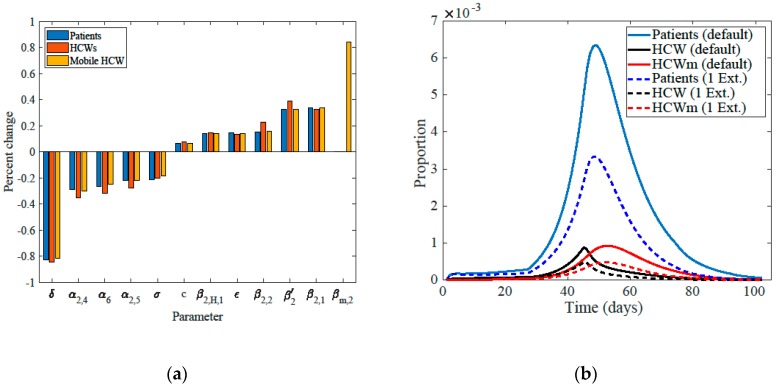
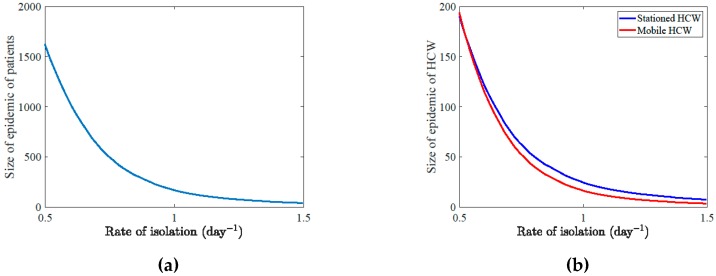
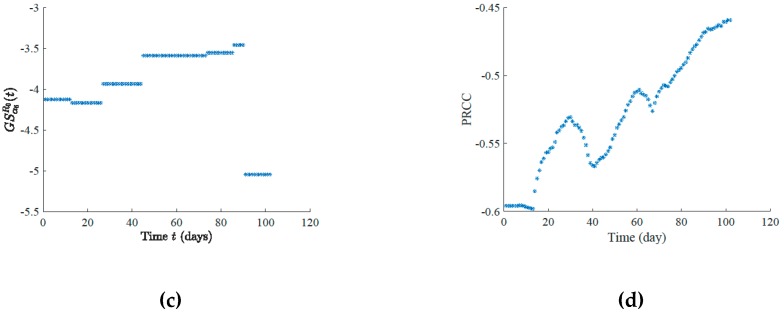
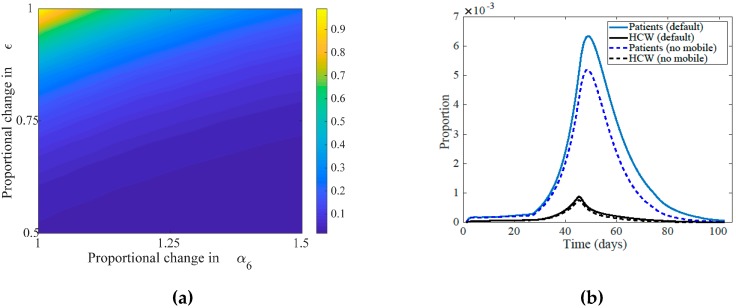
Middle East respiratory syndrome coronavirus (MERS-CoV) is an emerging zoonotic coronavirus that has a tendency to cause significant healthcare outbreaks among patients with serious comorbidities. We analyzed hospital data from the MERS-CoV outbreak in King Abdulaziz Medical Center, Riyadh, Saudi Arabia, June-August 2015 using the susceptible-exposed-infectious-recovered (SEIR) ward transmission model. The SEIR compartmental model considers several areas within the hospital where transmission occurred. We use a system of ordinary differential equations that incorporates the following units: emergency department (ED), out-patient clinic, intensive care unit, and hospital wards, where each area has its own carrying capacity and distinguishes the transmission by three individuals in the hospital: patients, health care workers (HCW), or mobile health care workers. The emergency department, as parameterized has a large influence over the epidemic size for both patients and health care workers. Trend of the basic reproduction number (R0), which reached a maximum of 1.39 at the peak of the epidemic and declined to 0.92 towards the end, shows that until added hospital controls are introduced, the outbreak would continue with sustained transmission between wards. Transmission rates where highest in the ED, and mobile HCWs were responsible for large part of the outbreak.
Keywords: SEIR ward transmission model; basic reproduction number; healthcare MERS-CoV outbreak.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Control ECfDPa Severe Respiratory Disease Associated with Middle East Respiratory Syndrome Coronavirus (MERS-CoV) 21st Update. [(accessed on 1 September 2019)];2015 Oct 21; Available online: https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publicat....
-
- World Health Organization Middle East Respiratory Syndrome Coronavirus (MERS-CoV) [(accessed on 1 September 2019)];2018 Available online: http://www.who.int/emergencies/mers-cov/en/
-
- Assiri A., Al-Tawfiq J.A., Al-Rabeeah A., Al-Rabiah F., Al-Hajjar S., Al-Barrak A., Flemban H., Al-Nassir W.N., Balkhy H.H., Al-Hakeem R.F., et al. Epidemiological, demographic, and clinical characteristics of 47 cases of Middle East respiratory syndrome coronavirus disease from Saudi Arabia: A descriptive study. Lancet Infect. Dis. 2013;13:752–761. doi: 10.1016/S1473-3099(13)70204-4. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
