

Provider Contributions to Disparities in Mental Health Care
- PMID: 32340593
- PMCID: PMC7590958
- DOI: 10.1176/appi.ps.201800500
Provider Contributions to Disparities in Mental Health Care
Abstract
Objective: Disparities in diagnosis of mental health problems and in access to treatment among racial-ethnic groups are apparent across different behavioral conditions, particularly in the quality of treatment for depression. This study aimed to determine how much disparities differ across providers.
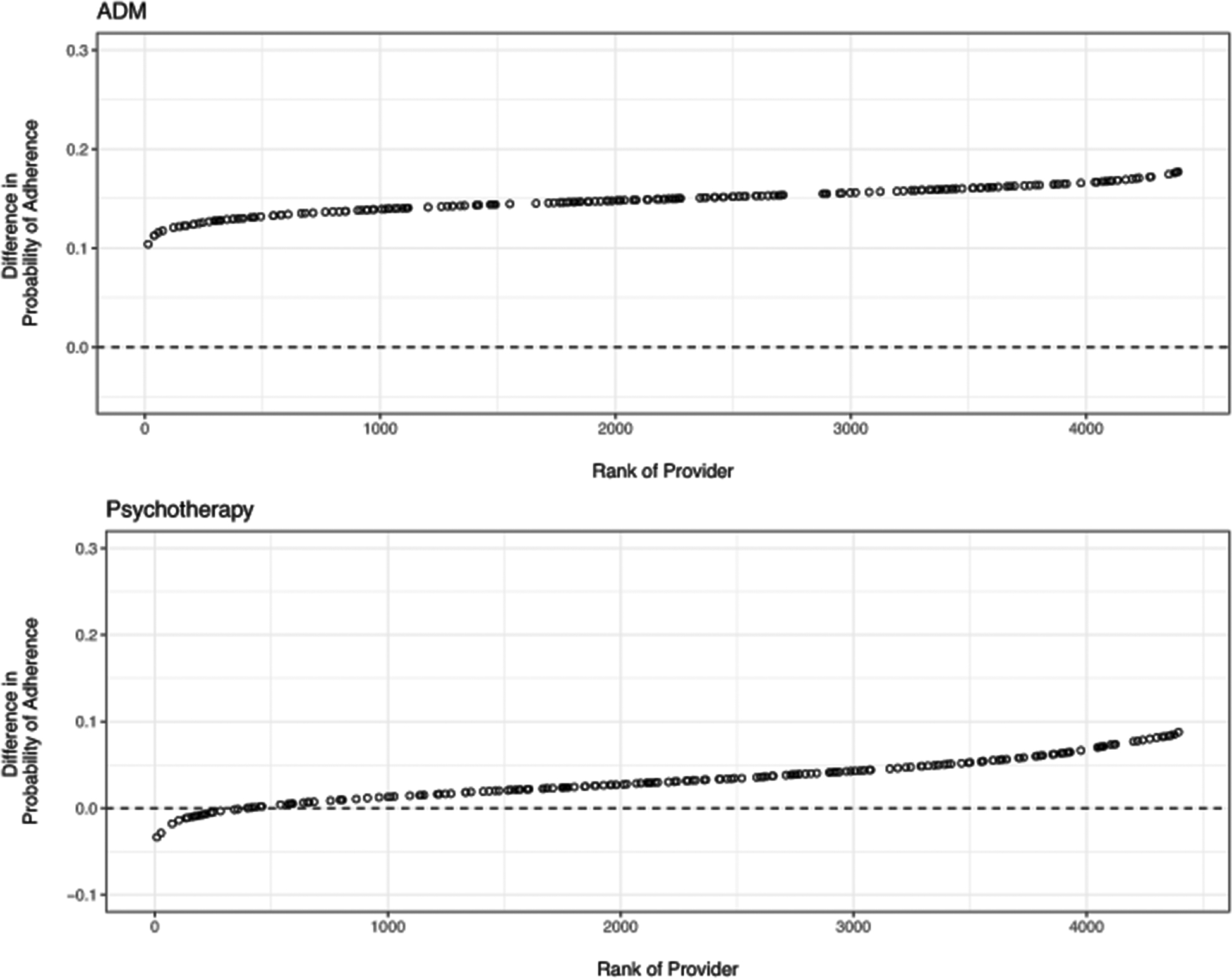
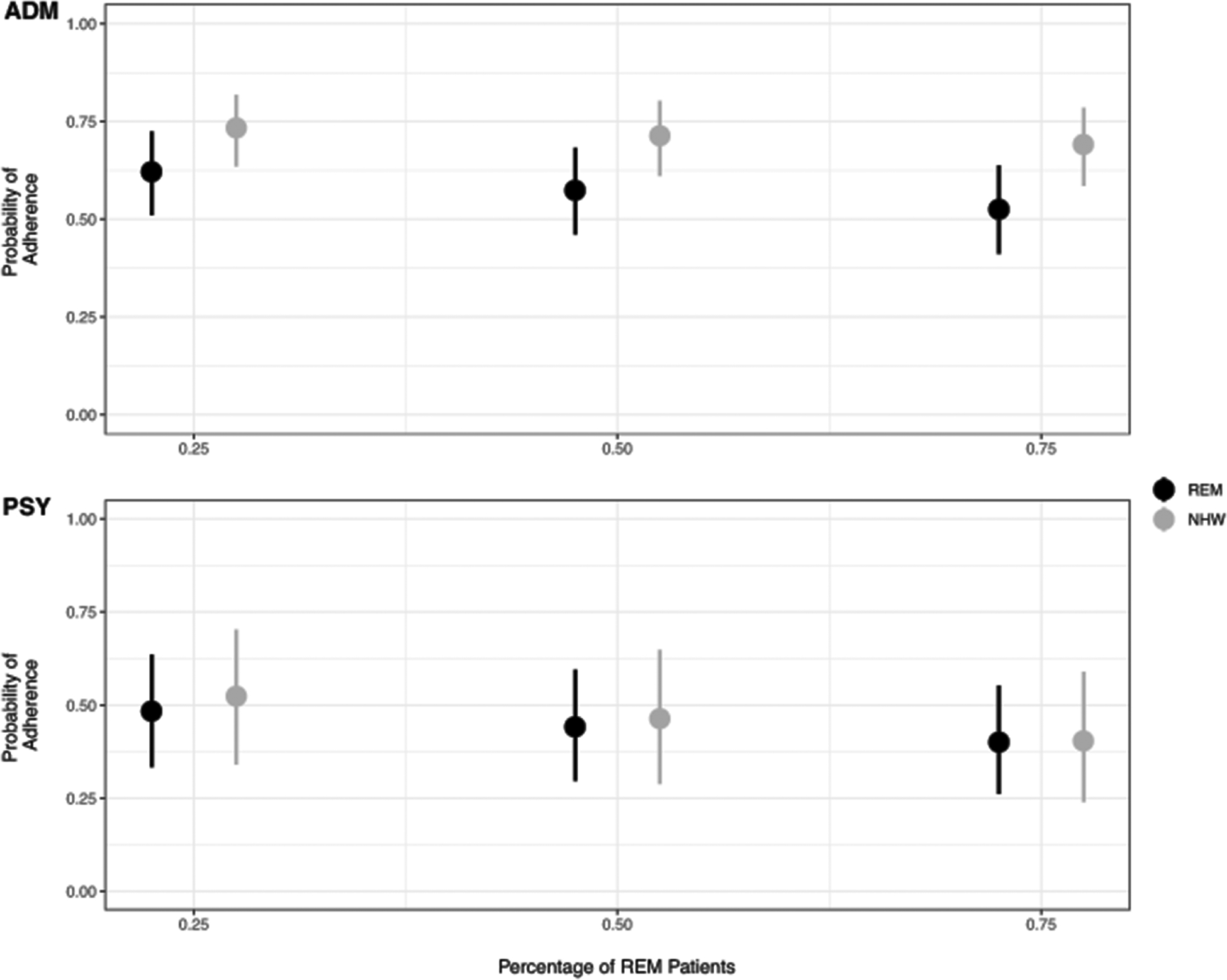
Methods: Bayesian mixed-effects models were used to estimate whether disparities in patient adherence to antidepressant medication (N=331,776) or psychotherapy (N=275,095) were associated with specific providers. Models also tested whether providers who achieved greater adherence to treatment, on average, among non-Hispanic white patients than among patients from racial-ethnic minority groups attained lower disparities and whether the percentage of patients from racial-ethnic minority groups in a provider caseload was associated with disparities.
Results: Disparities in adherence to both antidepressant medication and psychotherapy were associated with the provider. Provider performance with non-Hispanic white patients was negatively correlated with provider-specific disparities in adherence to psychotherapy but not to antidepressants. A higher proportion of patients from racial-ethnic minority groups in a provider's caseload was associated with lower adherence among non-Hispanic white patients, lower disparities in adherence to psychotherapy, and greater disparities in adherence to antidepressant medication.
Conclusions: Adherence to depression treatment among a provider's patients from racial-ethnic minority groups was related to adherence among that provider's non-Hispanic white patients, but evidence also suggested provider-specific disparities. Efforts among providers to decrease disparities might focus on improving the general skill of providers who treat more patients from racial-ethnic minority groups as well as offering culturally based training to providers with notable disparities.
Keywords: Bayesian multilevel modeling; adherence; cross-cultural issues; cultural competence; provider effects; racial-ethnic mental health disparities; treatment adherence.
Figures
References
-
- Centers for Disease Control and Prevention. CDC health disparities and inequalities report-United States, 2013. Foreword. MMWR supplements. https://www.cdc.gov/mmwr/pdf/other/su6203.pdf. Published November 2013. Accessed March 2017. - PubMed
-
- US Department of Health and Human Services. Disparities in healthcare quality among racial and ethnic minority groups. 2011. Washington, DC: Department of Health and Human Services.
-
- Institute of Medicine. Unequal treatment: Confronting racial and ethnic disparities in health care (full printed version). 2002. Washington, DC: National Academies Press. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
