

Locoregional delivery of CAR T cells to the cerebrospinal fluid for treatment of metastatic medulloblastoma and ependymoma
- PMID: 32341580
- PMCID: PMC8815773
- DOI: 10.1038/s41591-020-0827-2
Locoregional delivery of CAR T cells to the cerebrospinal fluid for treatment of metastatic medulloblastoma and ependymoma
Erratum in
-
Author Correction: Locoregional delivery of CAR T cells to the cerebrospinal fluid for treatment of metastatic medulloblastoma and ependymoma.Nat Med. 2021 Jun;27(6):1117-1120. doi: 10.1038/s41591-021-01362-1. Nat Med. 2021. PMID: 34045740 No abstract available.
Abstract
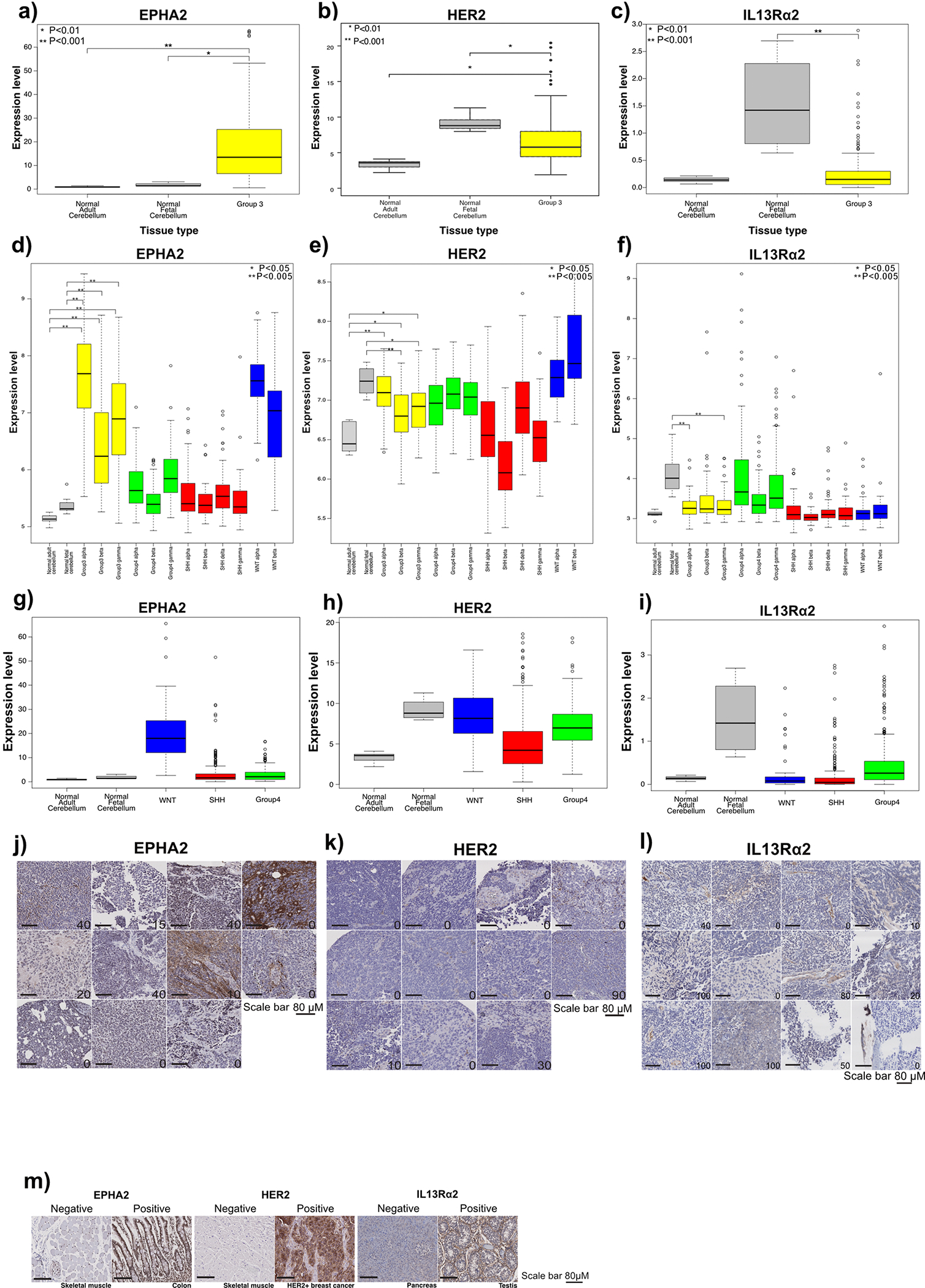
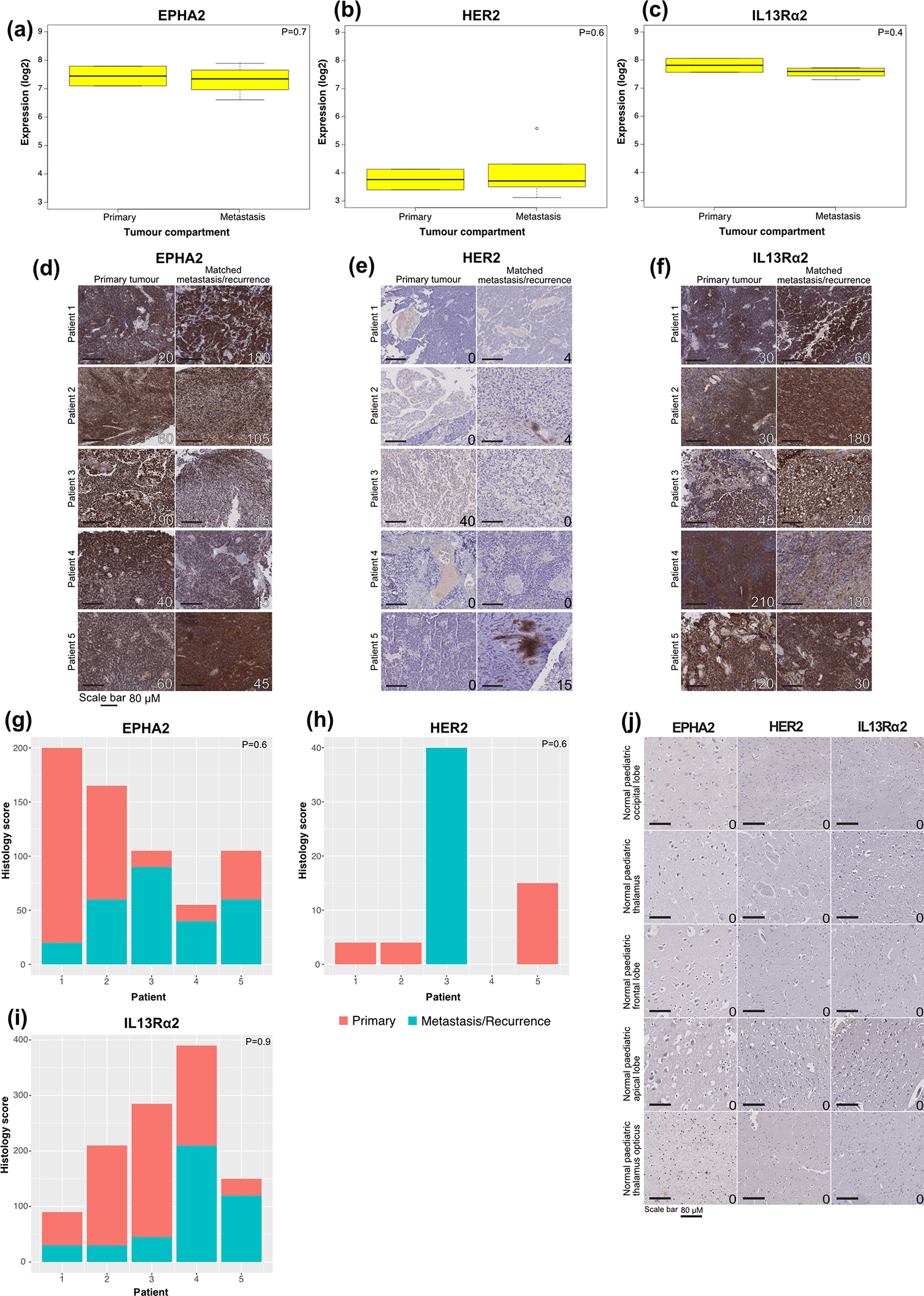
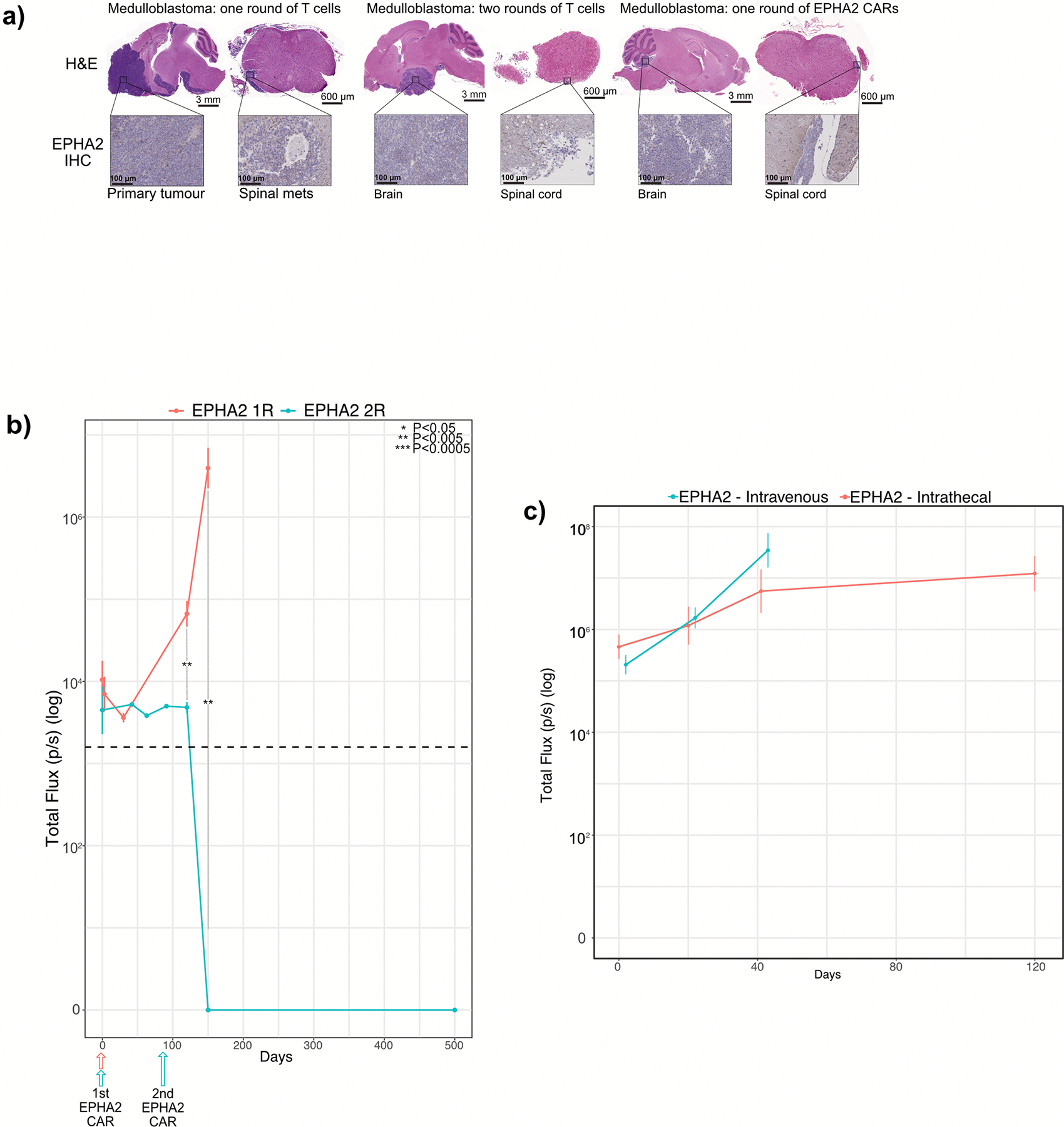
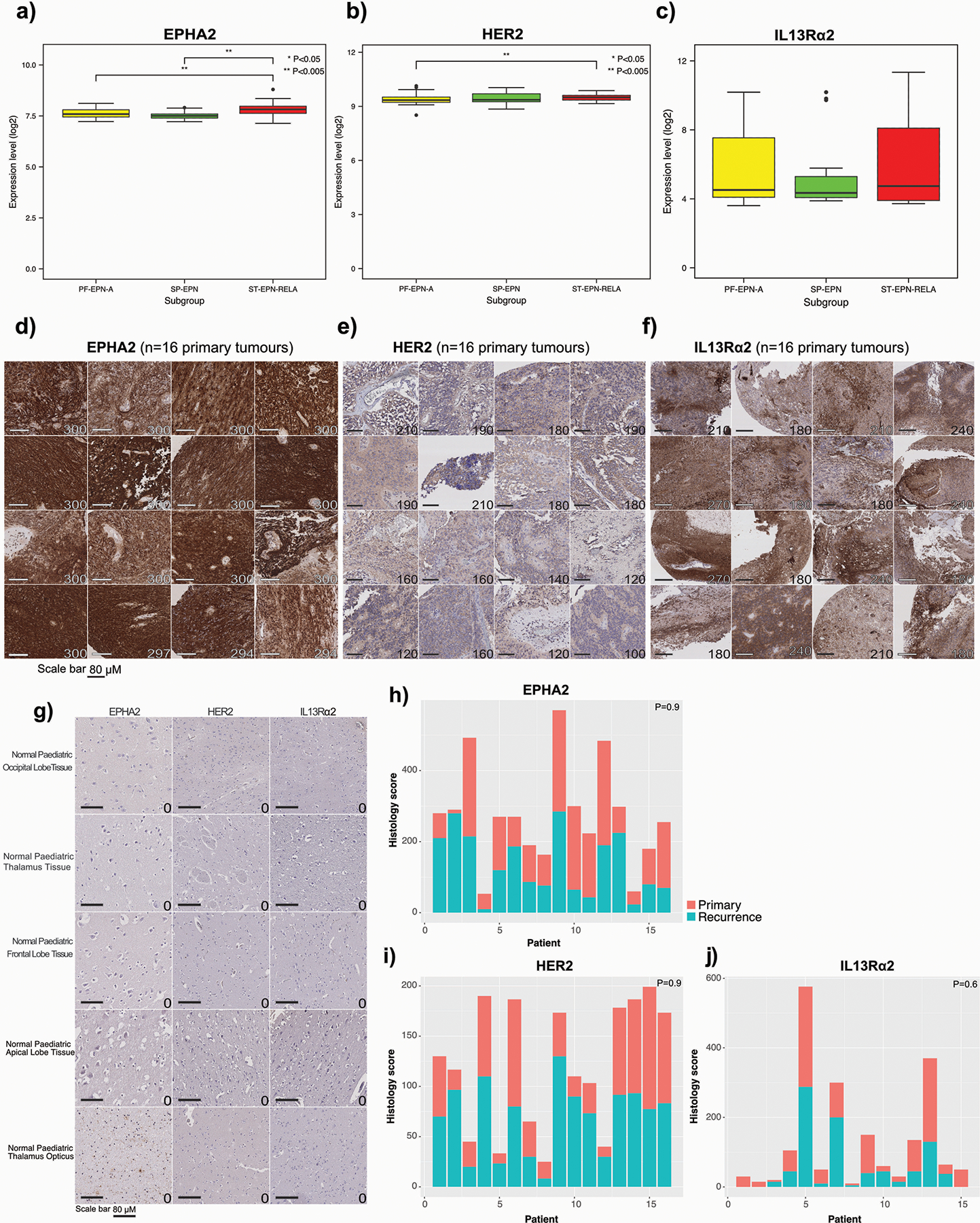
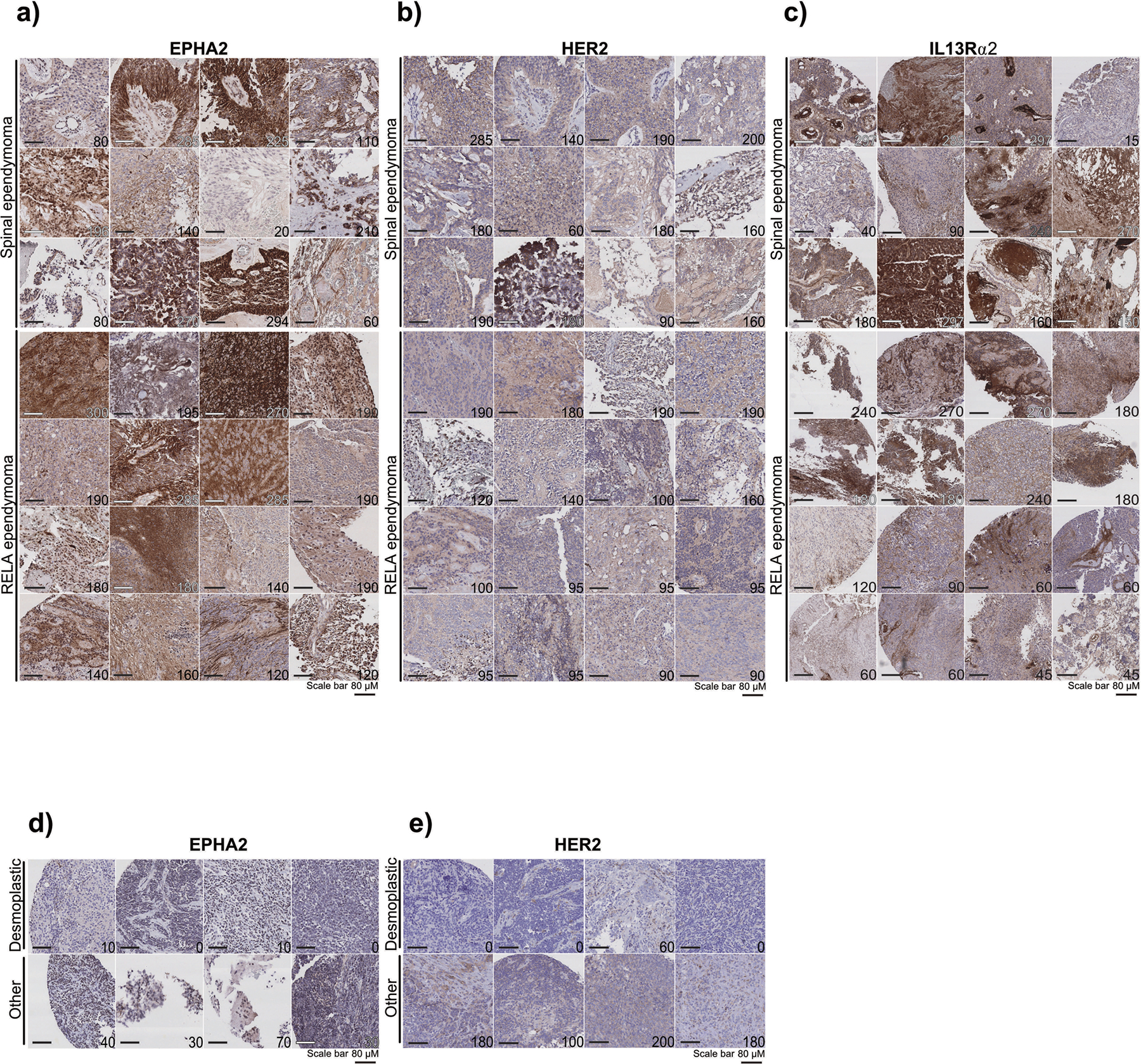
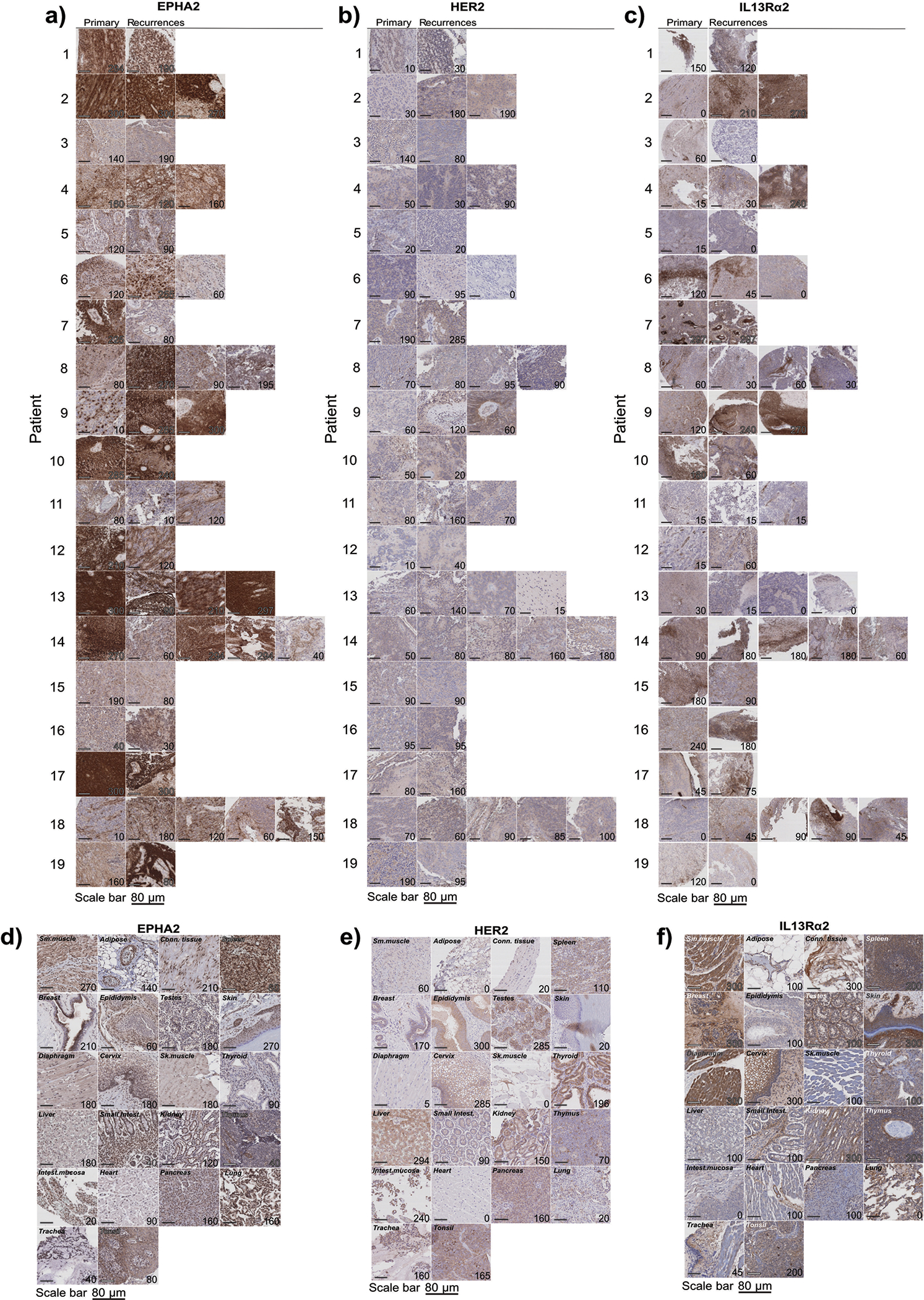
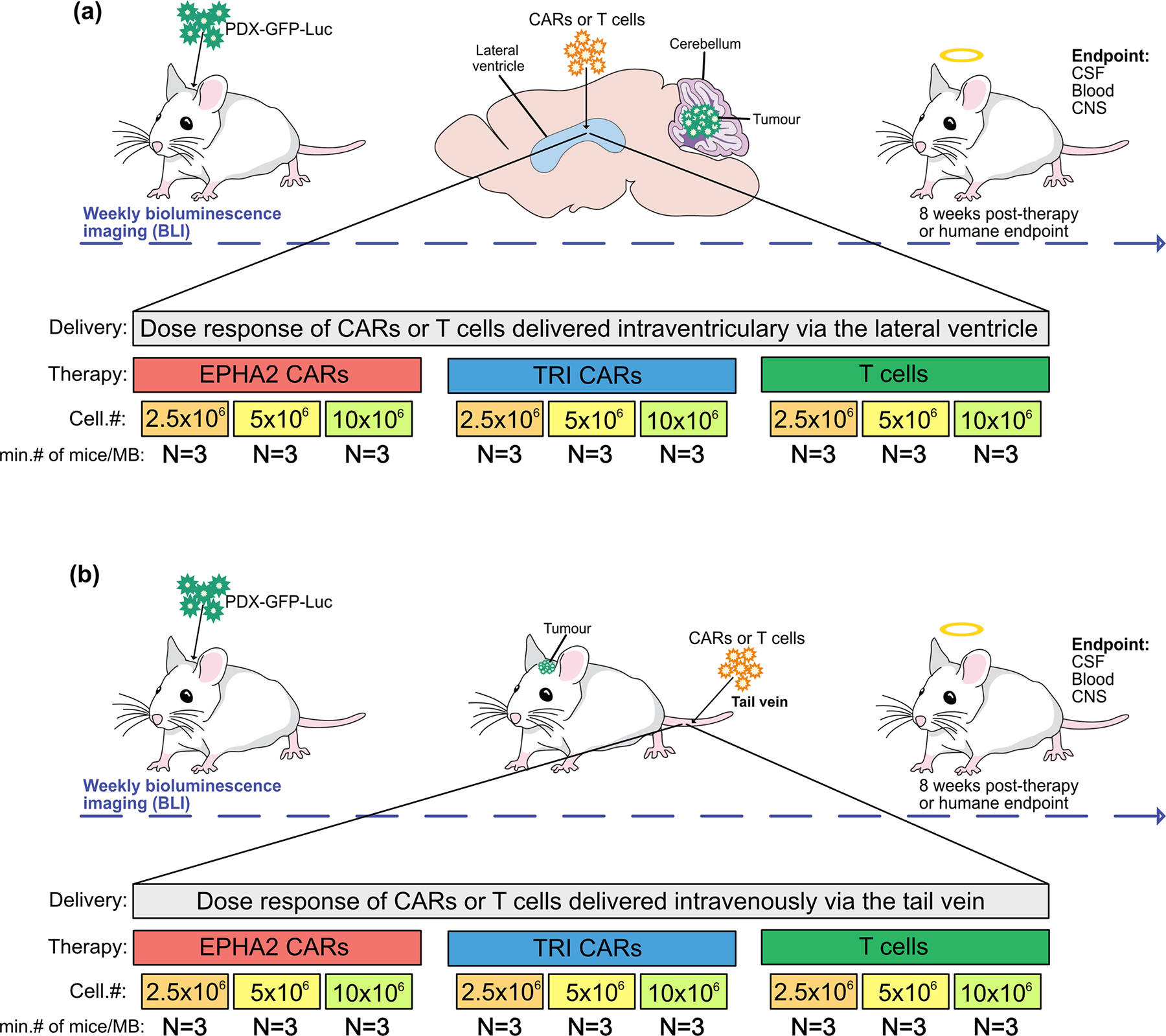
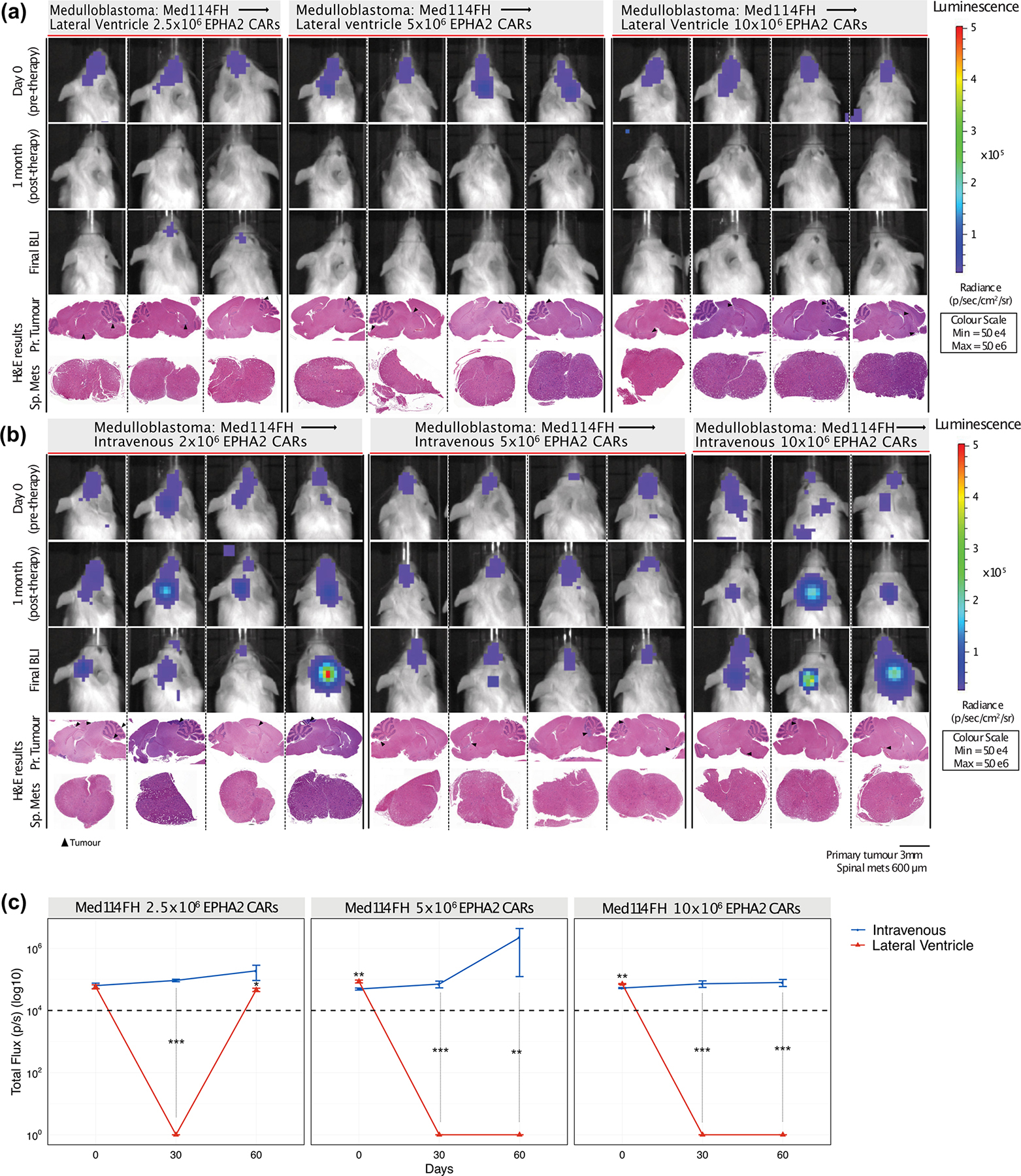
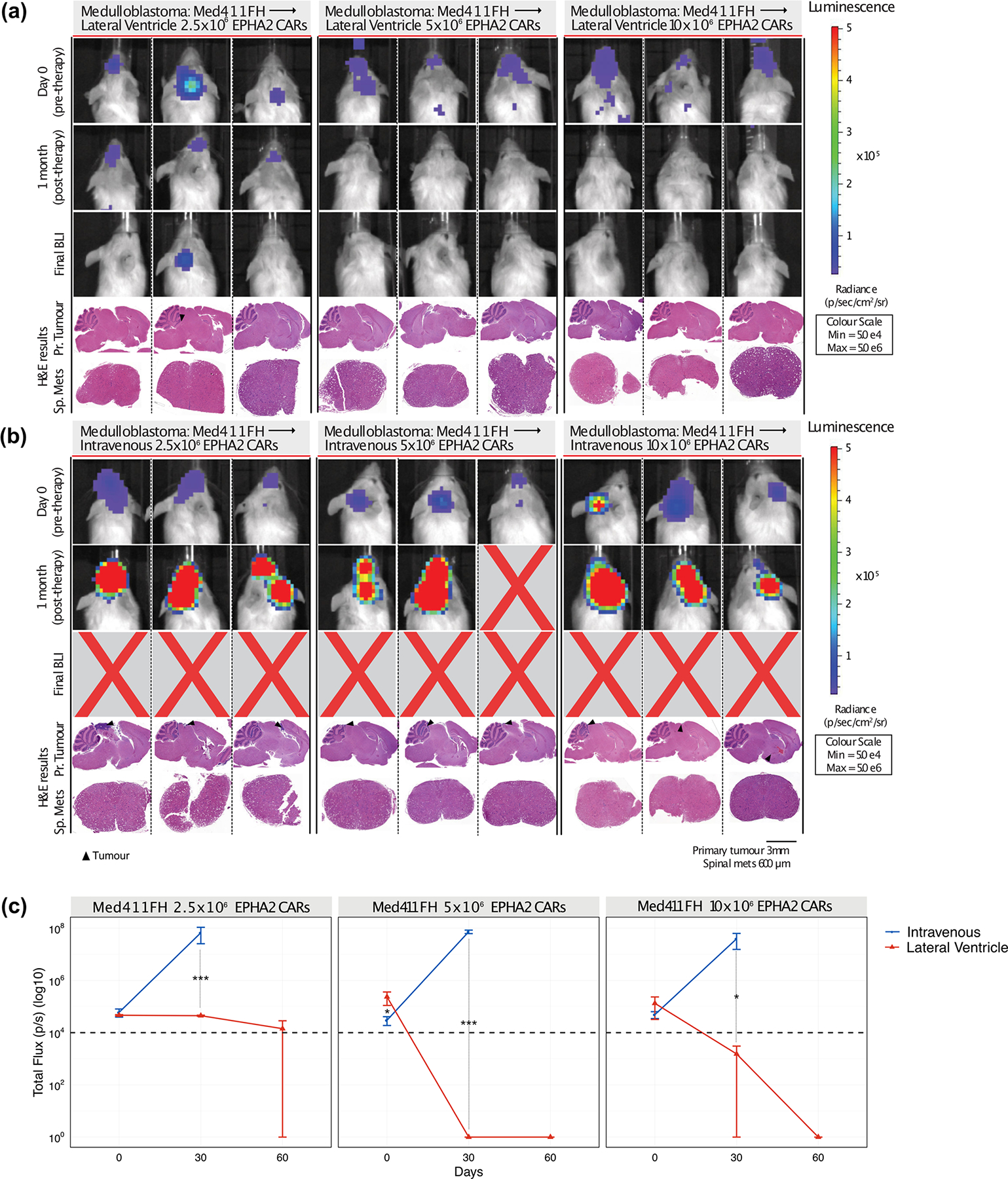
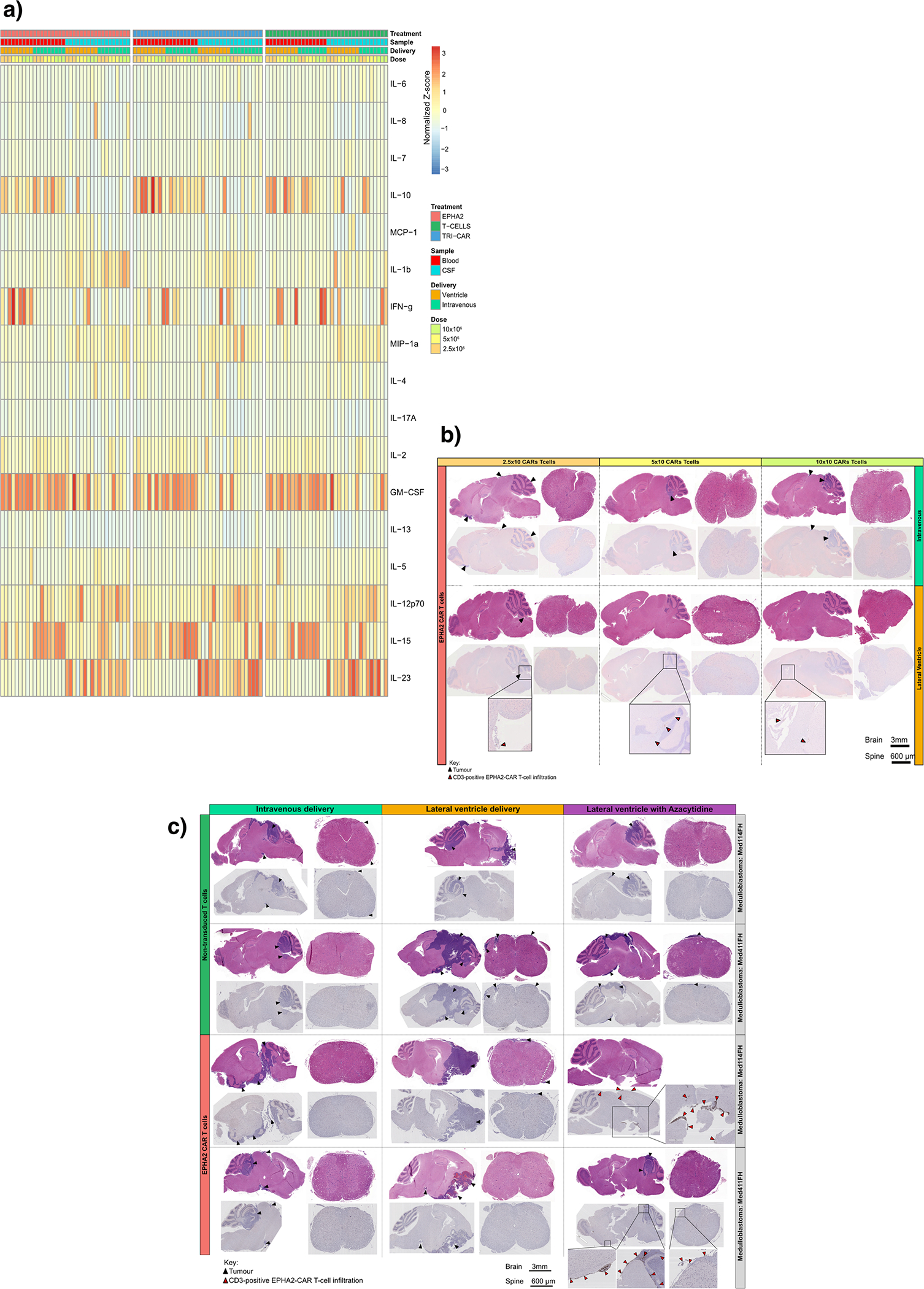
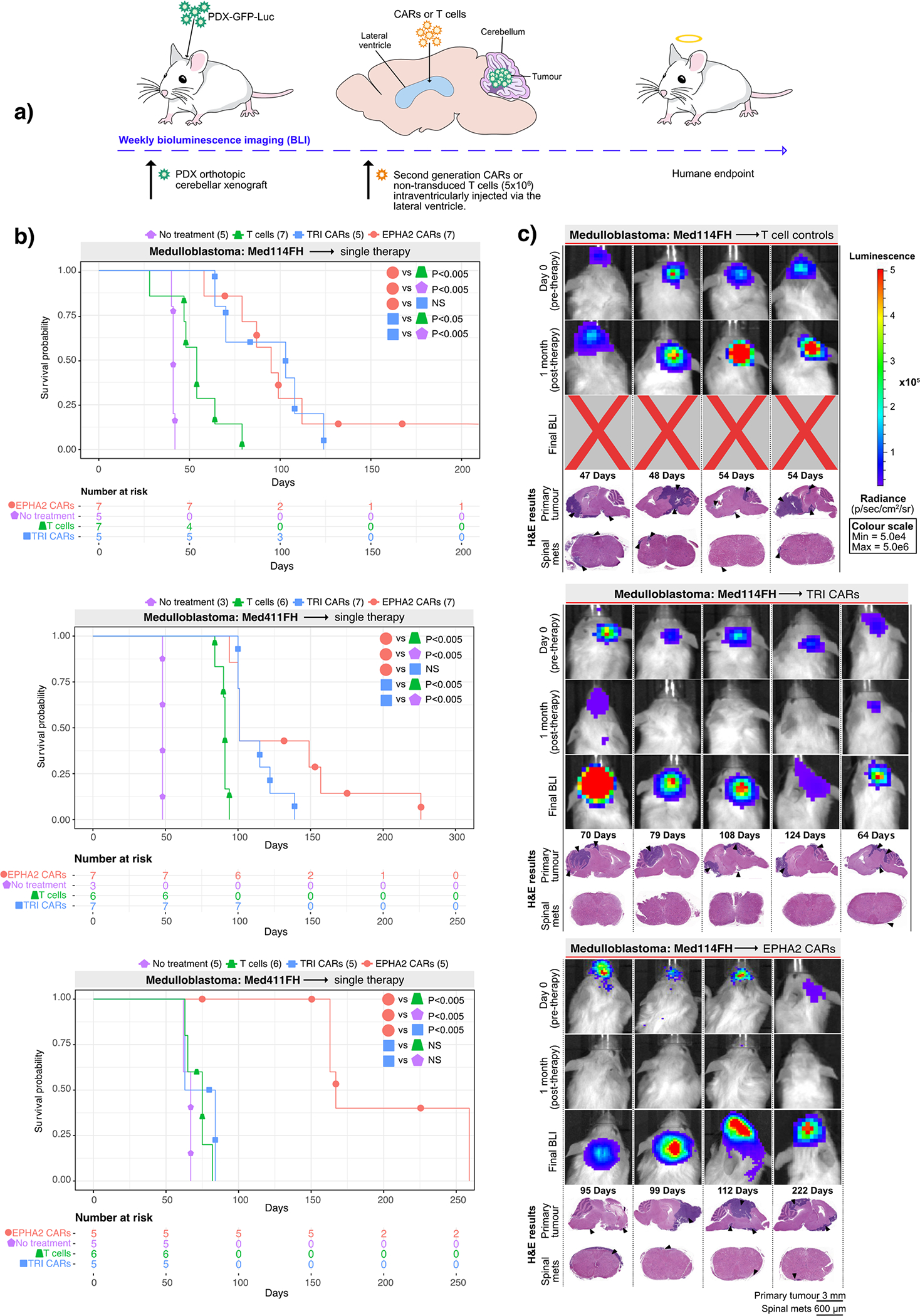
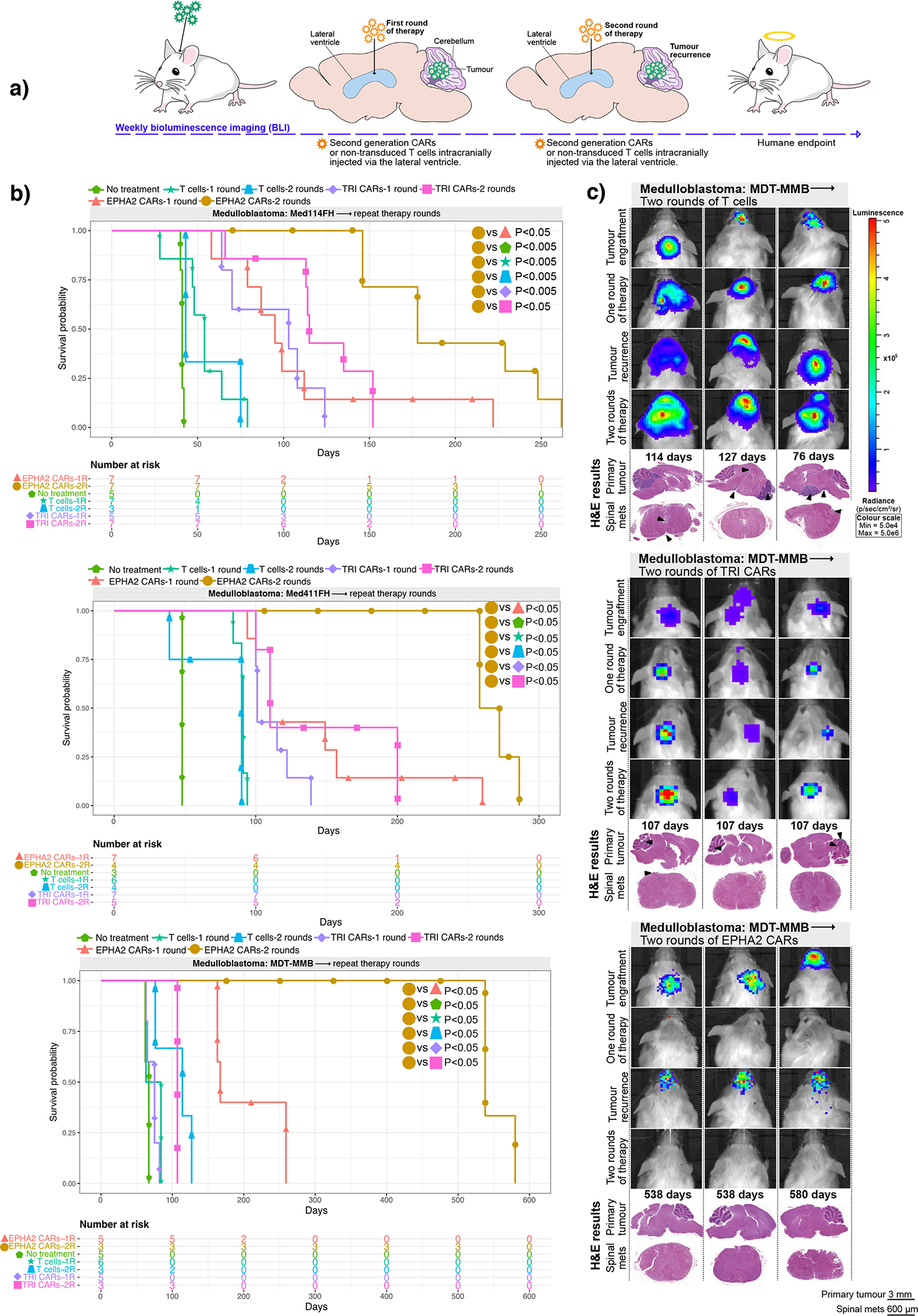
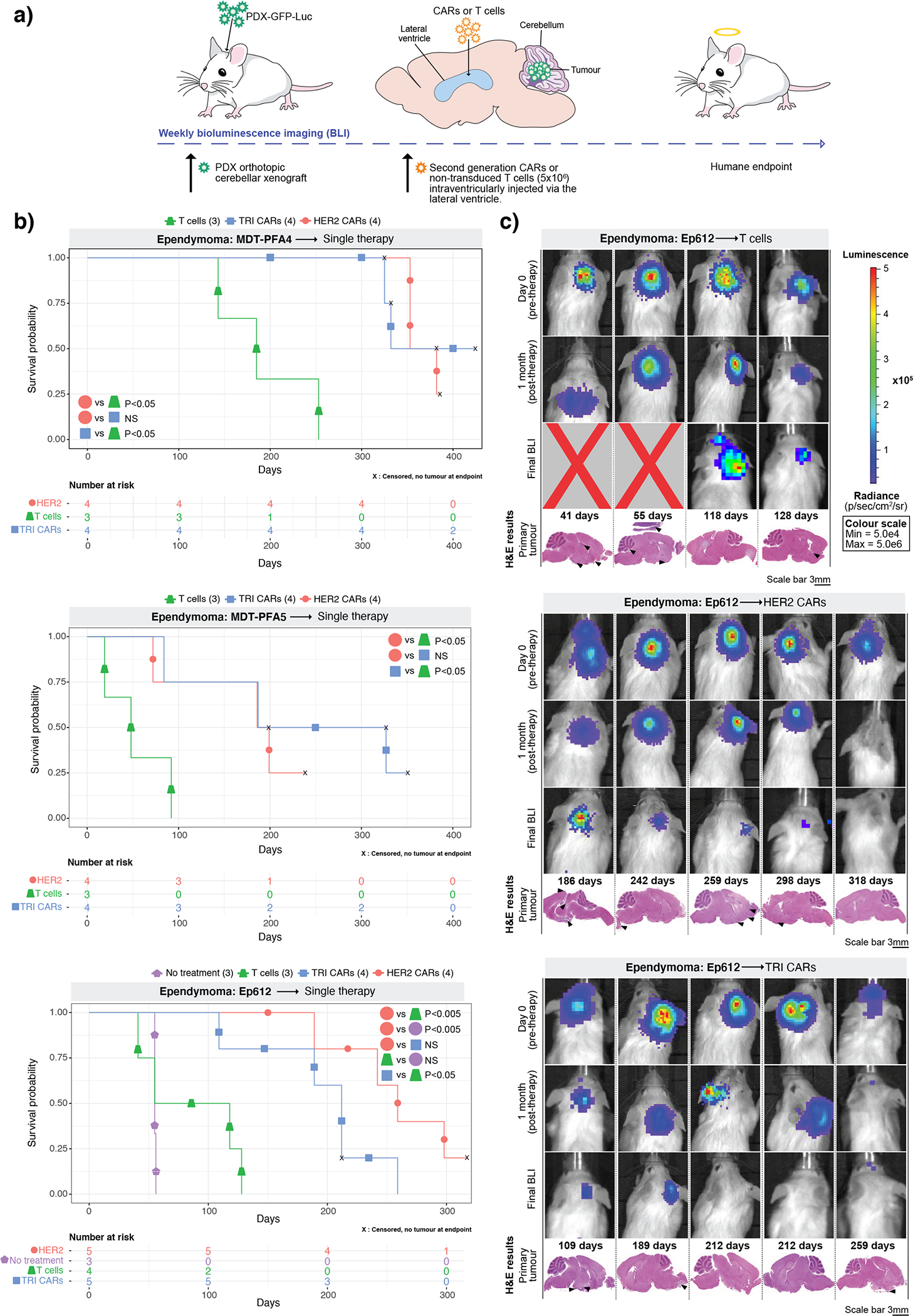
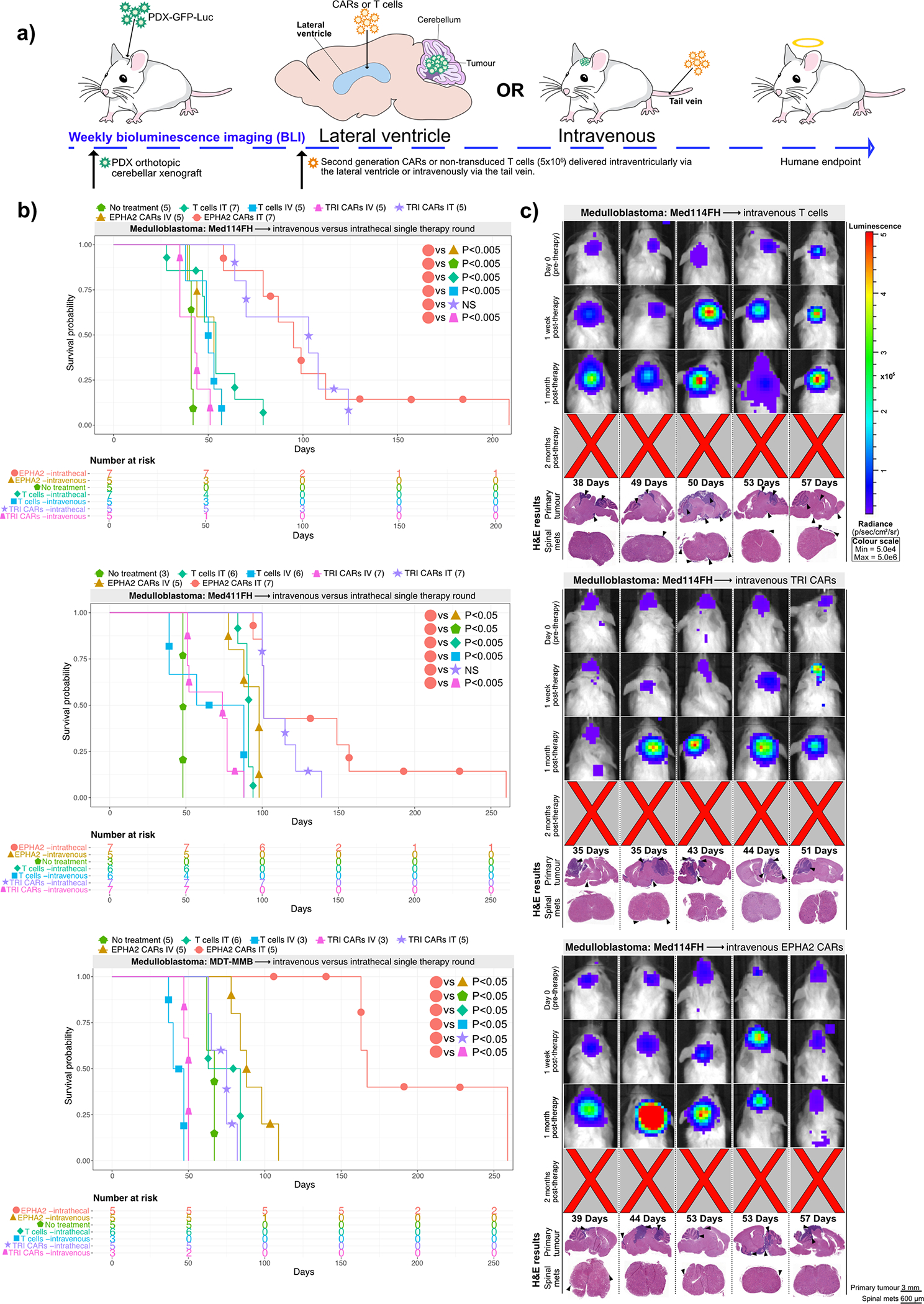
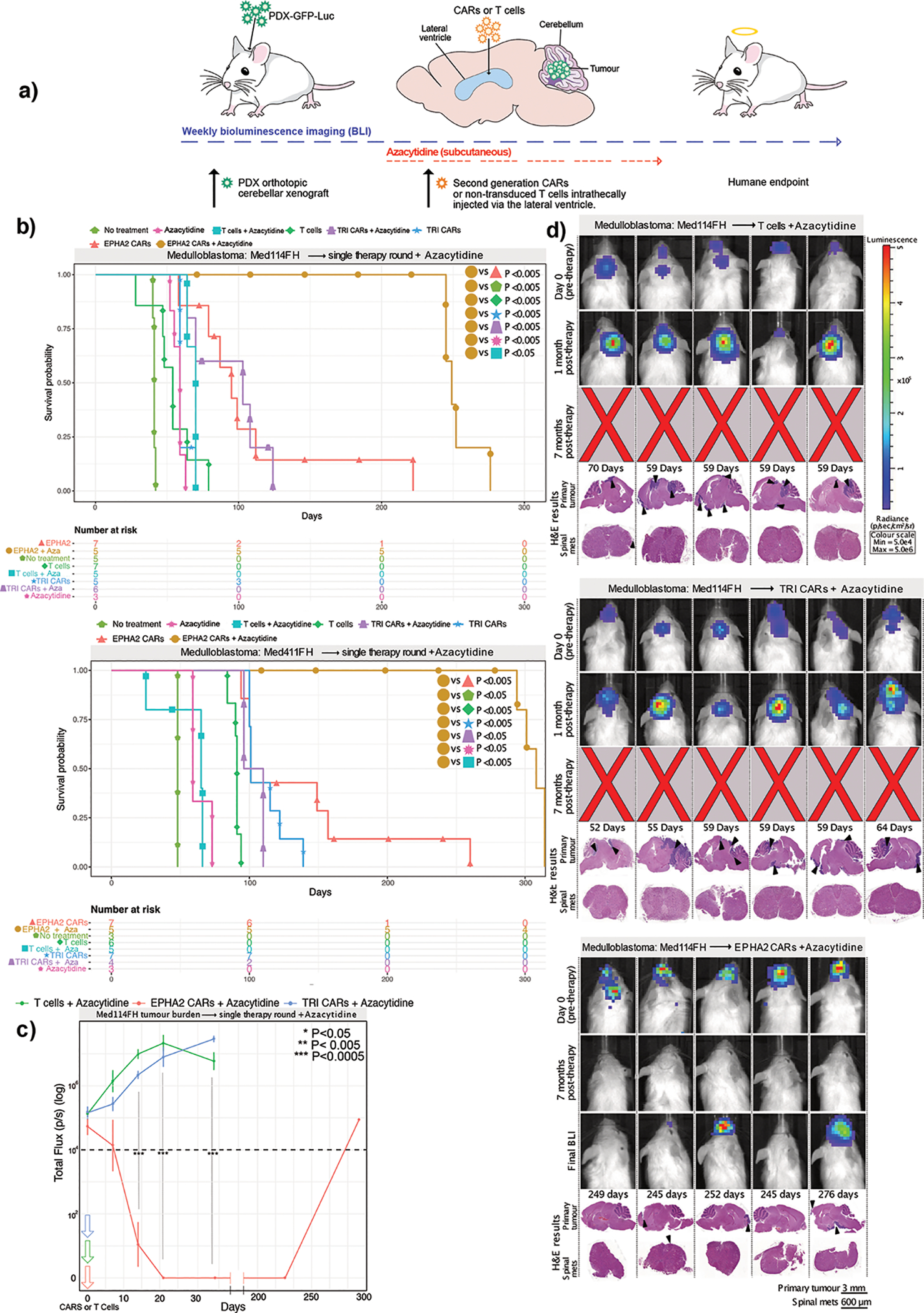
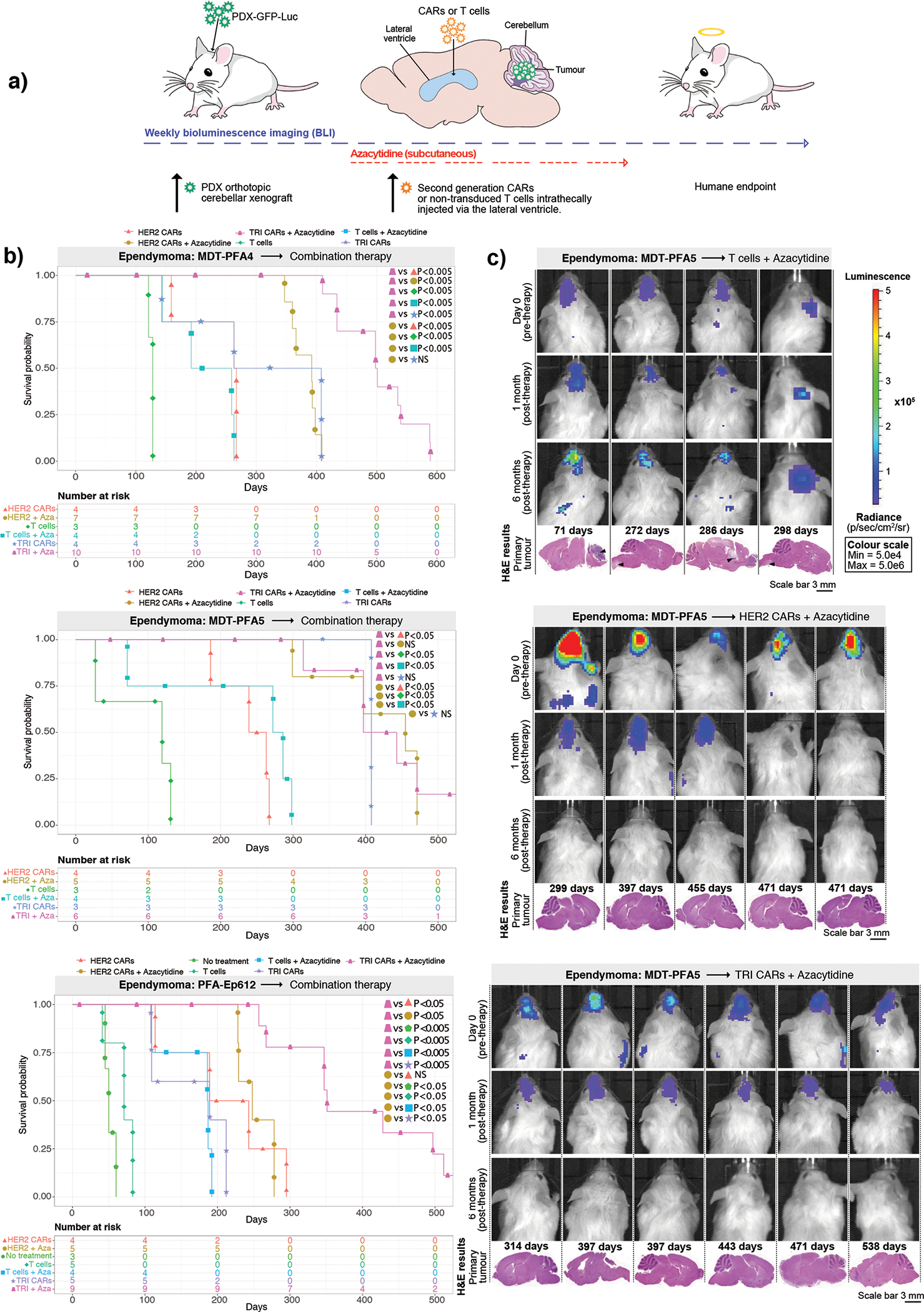
Recurrent medulloblastoma and ependymoma are universally lethal, with no approved targeted therapies and few candidates presently under clinical evaluation. Nearly all recurrent medulloblastomas and posterior fossa group A (PFA) ependymomas are located adjacent to and bathed by the cerebrospinal fluid, presenting an opportunity for locoregional therapy, bypassing the blood-brain barrier. We identify three cell-surface targets, EPHA2, HER2 and interleukin 13 receptor α2, expressed on medulloblastomas and ependymomas, but not expressed in the normal developing brain. We validate intrathecal delivery of EPHA2, HER2 and interleukin 13 receptor α2 chimeric antigen receptor T cells as an effective treatment for primary, metastatic and recurrent group 3 medulloblastoma and PFA ependymoma xenografts in mouse models. Finally, we demonstrate that administration of these chimeric antigen receptor T cells into the cerebrospinal fluid, alone or in combination with azacytidine, is a highly effective therapy for multiple metastatic mouse models of group 3 medulloblastoma and PFA ependymoma, thereby providing a rationale for clinical trials of these approaches in humans.
Conflict of interest statement
Competing interests statement
The authors declare no competing interests.
Figures
References
Methods only references
-
- Azemar M et al. Regression of Cutaneous Tumor Lesions in Patients Intratumorally Injected with Recombinant Single-chain Antibody-toxic Targted to ErbB2/HER2. Breats Cancer Res. Treat 82, 155–164 (2003). - PubMed
-
- Ahmed N et al. Regression of experimental medulloblastoma following transfer of HER2-specific T cells. Cancer Res (2007). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
