

Ultrasound-induced molecular delivery to erythrocytes using a microfluidic system
- PMID: 32341725
- PMCID: PMC7176461
- DOI: 10.1063/1.5144617
Ultrasound-induced molecular delivery to erythrocytes using a microfluidic system
Abstract
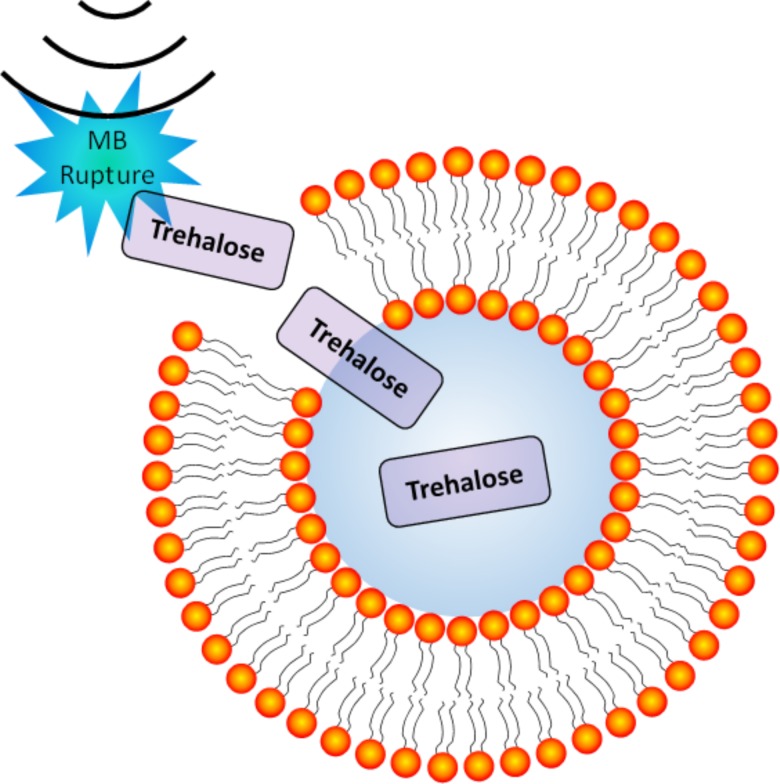
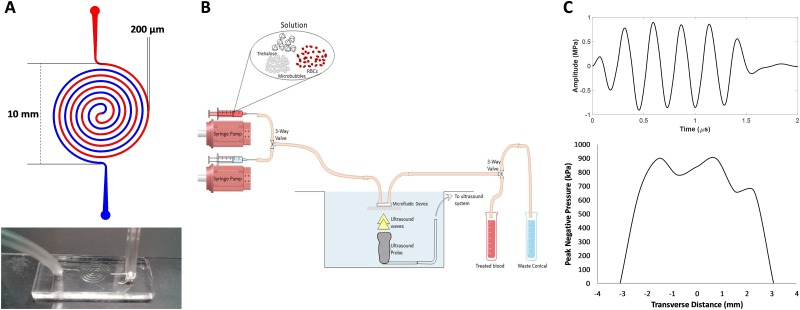
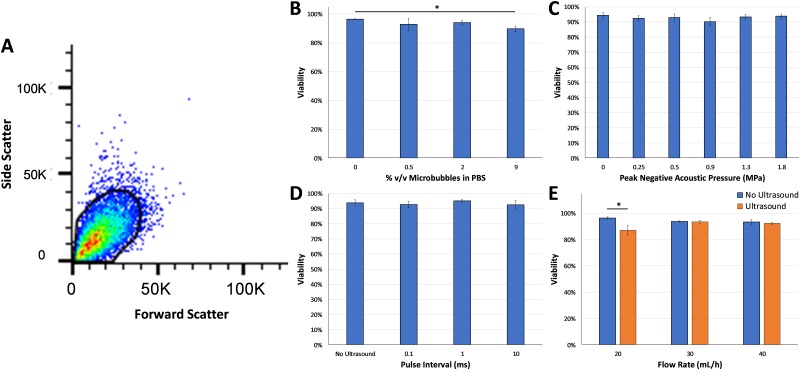
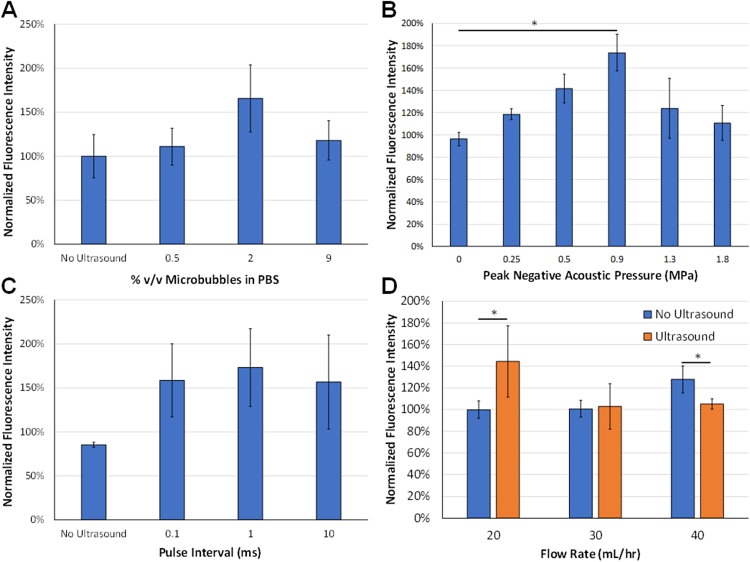
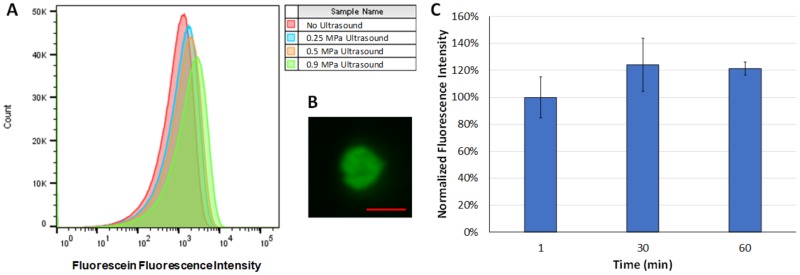
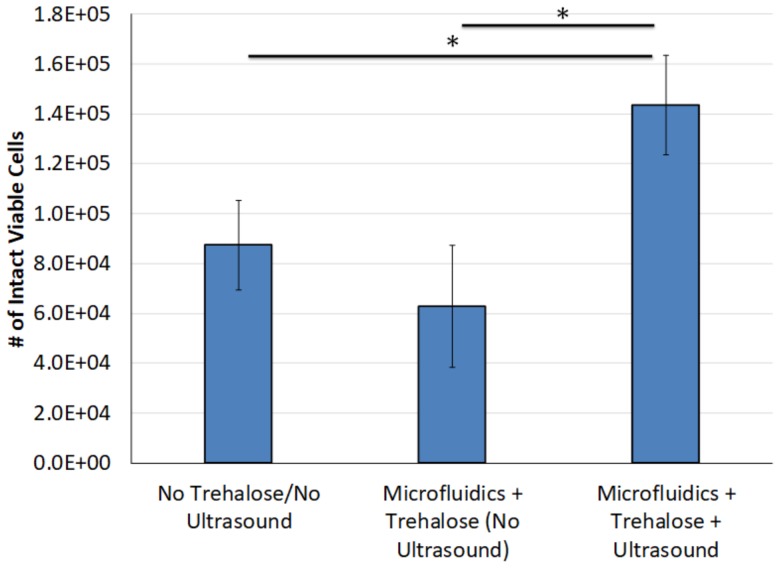
Preservation of erythrocytes in a desiccated state for storage at ambient temperature could simplify blood transfusions in austere environments, such as rural clinics, far-forward military operations, and during space travel. Currently, storage of erythrocytes is limited by a short shelf-life of 42 days at 4 °C, and long-term preservation requires a complex process that involves the addition and removal of glycerol from erythrocytes before and after storage at -80 °C, respectively. Natural compounds, such as trehalose, can protect cells in a desiccated state if they are present at sufficient levels inside the cell, but mammalian cell membranes lack transporters for this compound. To facilitate compound loading across the plasma membrane via ultrasound and microbubbles (sonoporation), a polydimethylsiloxane-based microfluidic device was developed. Delivery of fluorescein into erythrocytes was tested at various conditions to assess the effects of parameters such as ultrasound pressure, ultrasound pulse interval, microbubble dose, and flow rate. Changes in ultrasound pressure and mean flow rate caused statistically significant increases in fluorescein delivery of up to 73 ± 37% (p < 0.05) and 44 ± 33% (p < 0.01), respectively, compared to control groups, but no statistically significant differences were detected with changes in ultrasound pulse intervals. Following freeze-drying and rehydration, recovery of viable erythrocytes increased by up to 128 ± 32% after ultrasound-mediated loading of trehalose compared to control groups (p < 0.05). These results suggest that ultrasound-mediated molecular delivery in microfluidic channels may be a viable approach to process erythrocytes for long-term storage in a desiccated state at ambient temperatures.
Copyright © 2020 Author(s).
Figures
References
-
- Pfuntner A., Wier L. M., and Stocks C., “Most frequent procedures performed in U.S. hospitals, 2011: Statistical brief #165,” in Healthcare Cost and Utilization Project (HCUP) Statistical Briefs (Agency for Healthcare Research and Quality, Rockville, MD, 2006). - PubMed
-
- Izzo P. et al., “Erythrocytes stored in CPD SAG-mannitol: Evaluation of their deformability,” Clin. Hemorheol. Microcirc. 21(3–4), 335–339 (1999). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources