

Factors Associated With Neurobehavioral Complications in Pediatric Abdominal Organ Transplant Recipients Identified Using Computable Composite Definitions
- PMID: 32343104
- PMCID: PMC7888546
- DOI: 10.1097/PCC.0000000000002355
Factors Associated With Neurobehavioral Complications in Pediatric Abdominal Organ Transplant Recipients Identified Using Computable Composite Definitions
Abstract
Objectives: Neurologic complications occur in up to 40% of adult abdominal solid organ transplant recipients and are associated with increased mortality. Comparable pediatric data are sparse. This study describes the occurrence of neurologic and behavioral complications (neurobehavioral complications) in pediatric abdominal solid organ transplant recipients. We examine the association of these complications with length of stay, mortality, and tacrolimus levels.
Design: The electronic health record was interrogated for inpatient readmissions of pediatric abdominal solid organ transplant recipients from 2009 to 2017. A computable composite definition of neurobehavioral complication, defined using structured electronic data for neurologic and/or behavioral phenotypes, was created.
Setting: Quaternary children's hospital with an active transplant program.
Patients: Pediatric abdominal solid organ transplant recipients.
Interventions: None.
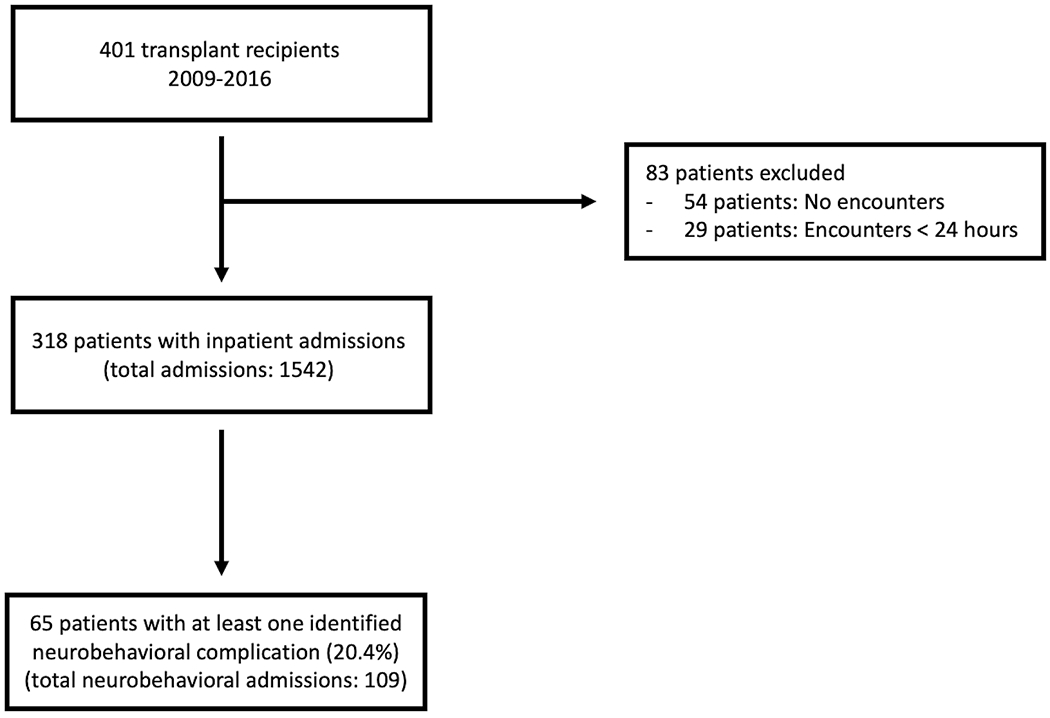
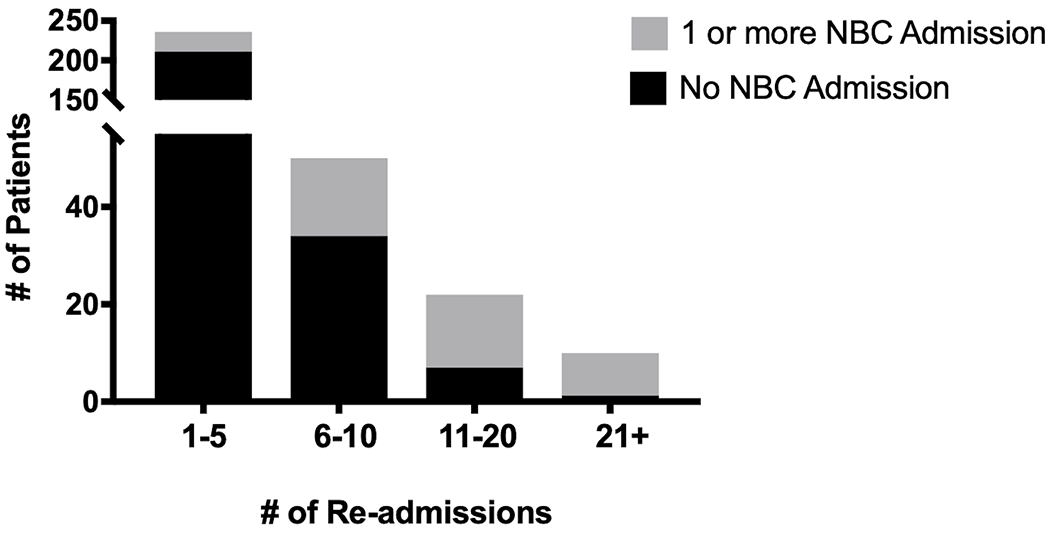
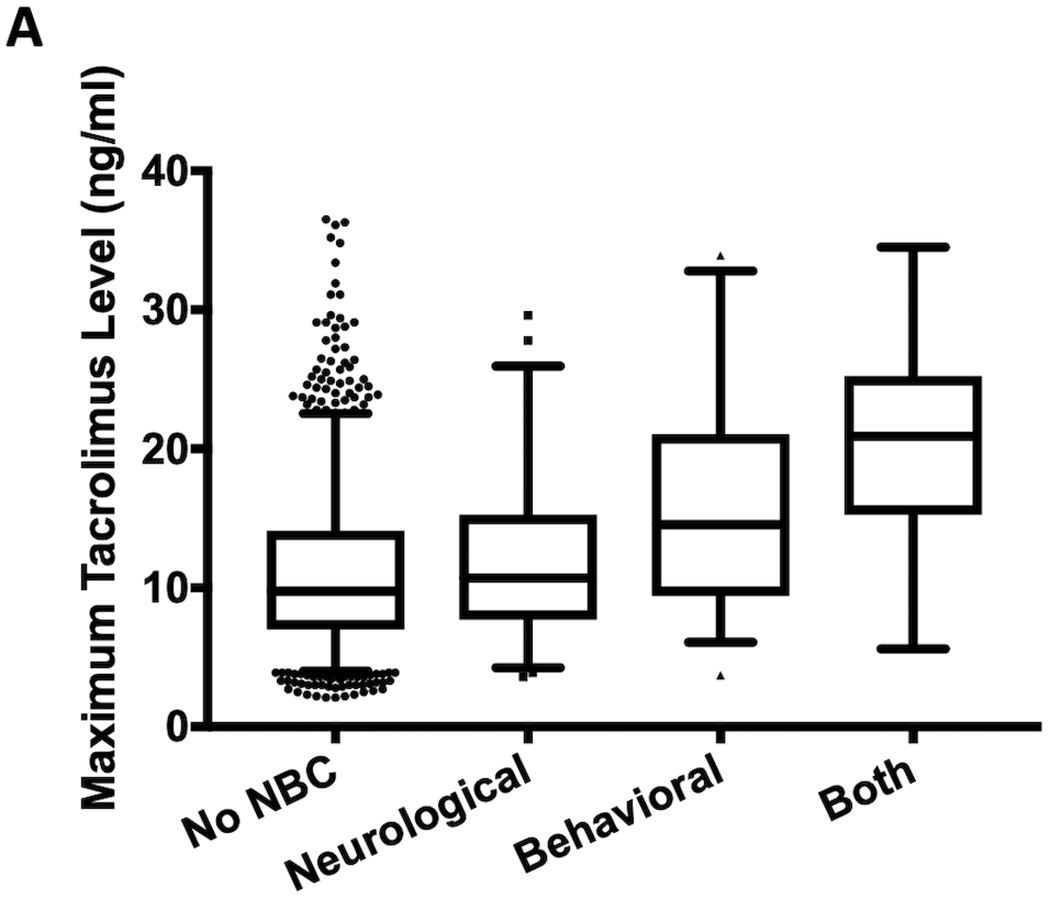
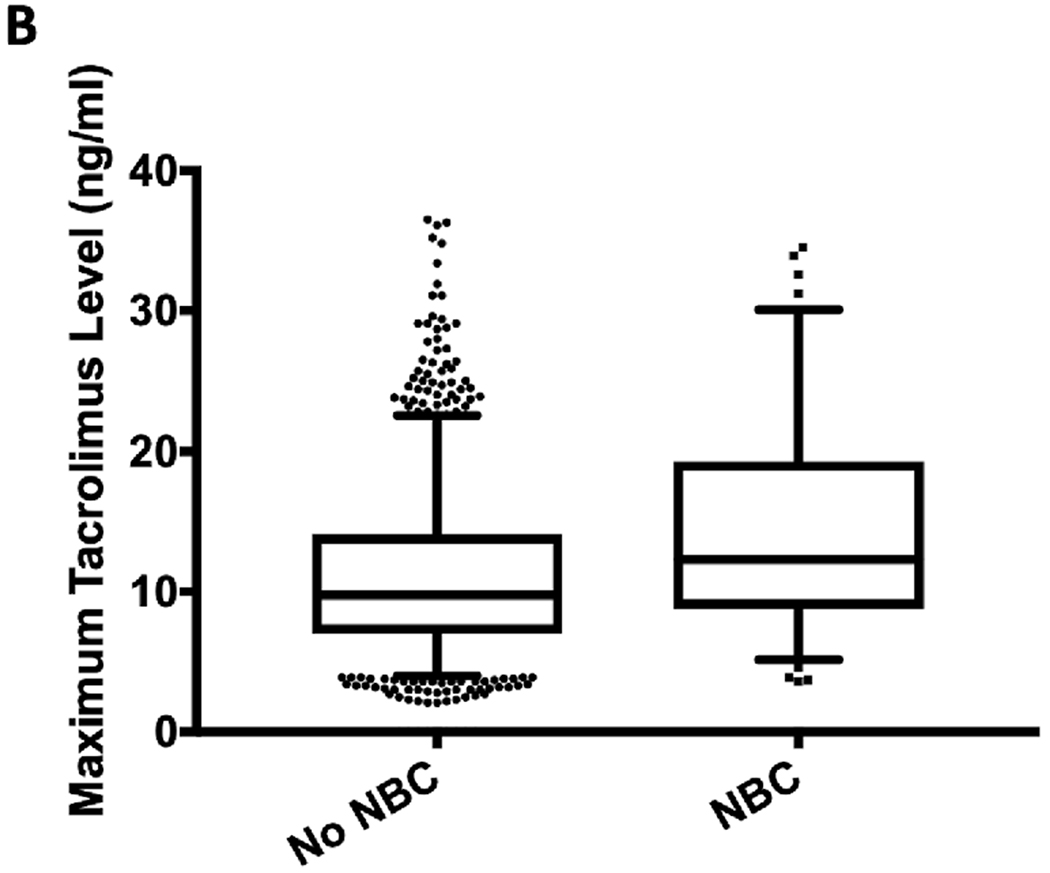
Measurements and main results: Computable phenotypes demonstrated a specificity 98.7% and sensitivity of 63.0% for identifying neurobehavioral complications. There were 1,542 readmissions among 318 patients, with 65 (20.4%) having at least one admission with a neurobehavioral complication (total 109 admissions). Median time from transplant to admission with neurobehavioral complication was 1.2 years (interquartile range, 0.52-2.28 yr). Compared to encounters without an identified neurobehavioral complication, encounters with a neurobehavioral complication were more likely to experience ICU admission (odds ratio, 3.9; 2.41-6.64; p < 0.001), have longer ICU length of stay (median 10.3 vs 2.2 d; p < 0.001) and hospital length of stay (8.9 vs 4.3 d; p < 0.001), and demonstrate higher maximum tacrolimus level (12.3 vs 9.8 ng/mL; p = 0.001). Patients with a neurobehavioral complication admission were more likely to die (odds ratio, 5.04; 1.49-17.09; p = 0.009). In a multivariable analysis, type of transplant, ICU admission, and tacrolimus levels were independently associated with the presence of a neurobehavioral complication.
Conclusions: Common electronic health record variables can be used to accurately identify neurobehavioral complications in the pediatric abdominal solid organ transplant population. Late neurobehavioral complications are associated with increased hospital resource utilization, mortality, and tacrolimus exposure. Additional studies are required to delineate the relationship between maximum tacrolimus level and neurobehavioral complications to guide therapeutic drug monitoring and dosing.
Figures
Comment in
-
Neurobehavioral Complications After Abdominal Organ Transplantation: Considering a Broader Phenotype and Care Plan.Pediatr Crit Care Med. 2020 Sep;21(9):837-838. doi: 10.1097/PCC.0000000000002401. Pediatr Crit Care Med. 2020. PMID: 32890084 No abstract available.
References
-
- Balderramo D, Prieto J, Cárdenas A, et al. Hepatic encephalopathy and post-transplant hyponatremia predict early calcineurin inhibitor-induced neurotoxicity after liver transplantation. Transpl Int 2011; 24: 812–819. - PubMed
-
- Colombari RC, de Ataíde EC, Udo EY, et al. Neurological complications prevalence and long-term survival after liver transplantation. Transplant Proc 2013; 45: 1126–1129. - PubMed
-
- Kim BS, Lee SG, Hwang S, et al. Neurologic complications in adult living donor liver transplant recipients. Clin Transplant 2007; 21: 544–547. - PubMed
-
- Rompianesi G, Montalti R, Cautero N, et al. Neurological complications after liver transplantation as a consequence of immunosuppression: univariate and multivariate analysis of risk factors. Transpl Int 2015; 28: 864–869. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
