

Staffing With Disease-Based Epidemiologic Indices May Reduce Shortage of Intensive Care Unit Staff During the COVID-19 Pandemic
- PMID: 32343514
- PMCID: PMC7173088
- DOI: 10.1213/ANE.0000000000004849
Staffing With Disease-Based Epidemiologic Indices May Reduce Shortage of Intensive Care Unit Staff During the COVID-19 Pandemic
Abstract
Background: Health care worker (HCW) safety is of pivotal importance during a pandemic such as coronavirus disease 2019 (COVID-19), and employee health and well-being ensure functionality of health care institutions. This is particularly true for an intensive care unit (ICU), where highly specialized staff cannot be readily replaced. In the light of lacking evidence for optimal staffing models in a pandemic, we hypothesized that staff shortage can be reduced when staff scheduling takes the epidemiology of a disease into account.
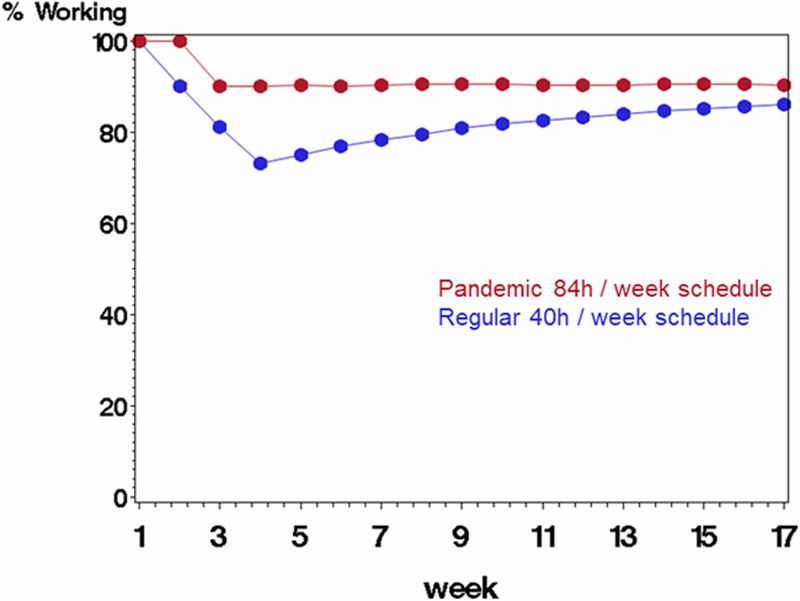
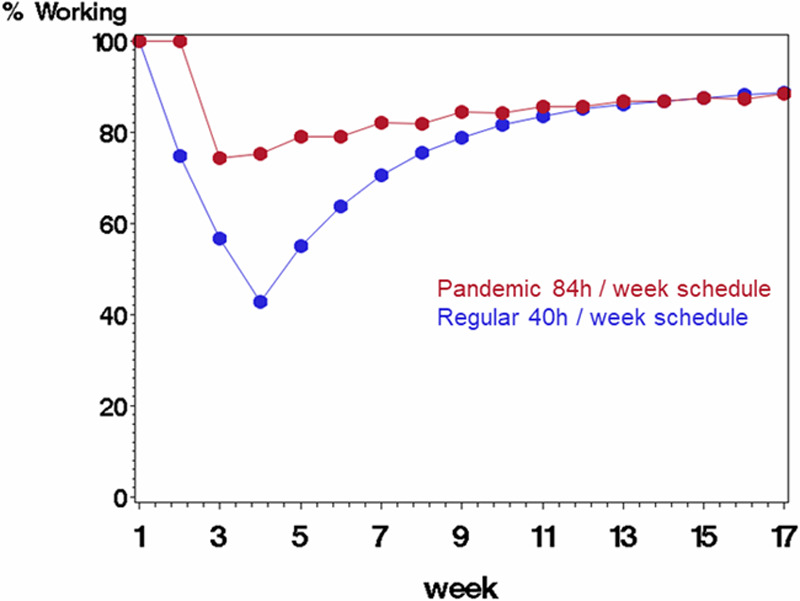
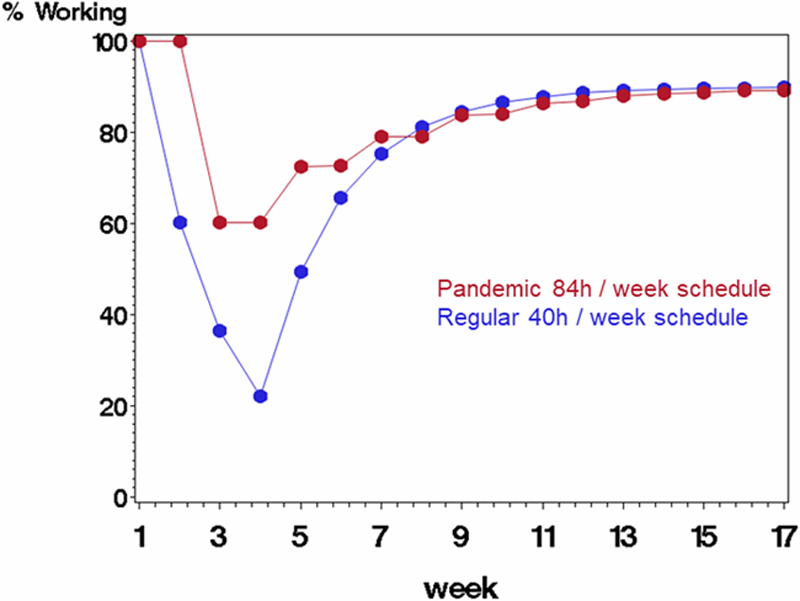
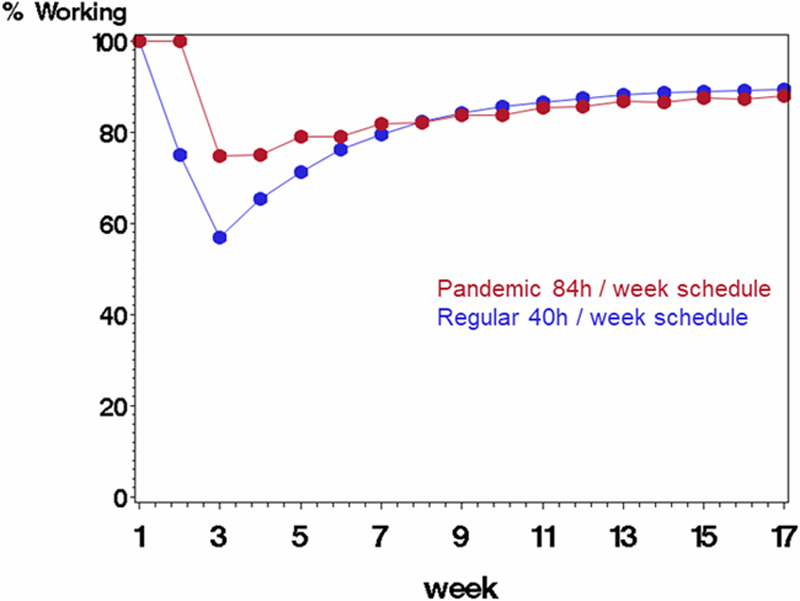
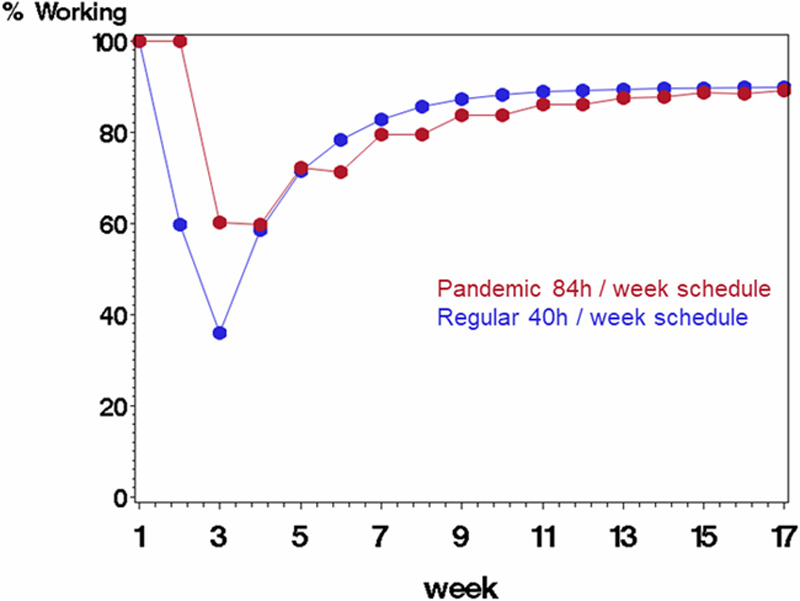
Methods: Various staffing models were constructed, and comprehensive statistical modeling was performed. A typical routine staffing model was defined that assumed full-time employment (40 h/wk) in a 40-bed ICU with a 2:1 patient-to-staff ratio. A pandemic model assumed that staff worked 12-hour shifts for 7 days every other week. Potential in-hospital staff infections were simulated for a total period of 120 days, with a probability of 10%, 25%, and 40% being infected per week when at work. Simulations included the probability of infection at work for a given week, of fatality after infection, and the quarantine time, if infected.
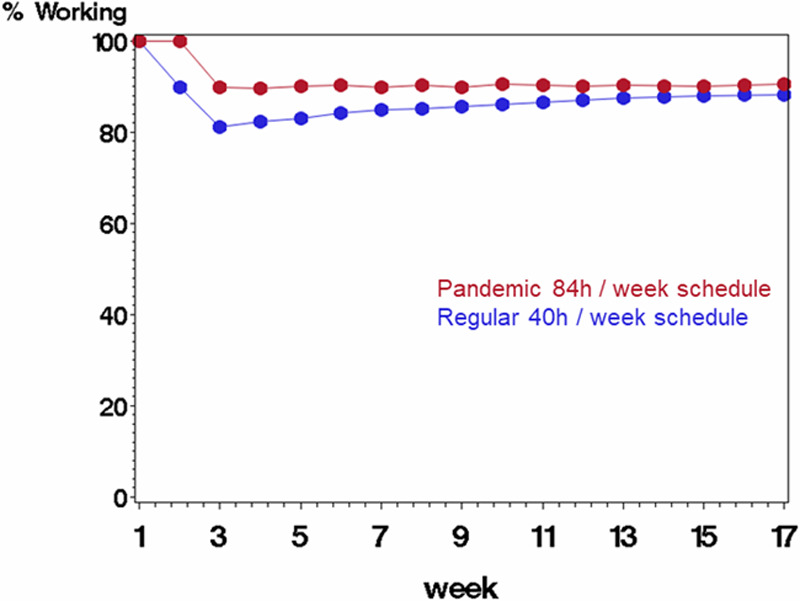
Results: Pandemic-adjusted staffing significantly reduced workforce shortage, and the effect progressively increased as the probability of infection increased. Maximum effects were observed at week 4 for each infection probability with a 17%, 32%, and 38% staffing reduction for an infection probability of 0.10, 0.25, and 0.40, respectively.
Conclusions: Staffing along epidemiologic considerations may reduce HCW shortage by leveling the nadir of affected workforce. Although this requires considerable efforts and commitment of staff, it may be essential in an effort to best maintain staff health and operational functionality of health care facilities and systems.
Conflict of interest statement
Conflicts of Interest: See Disclosures at the end of the article.
Figures
Comment in
-
Calculate the COVID-19 Equation With People's Energy as a Key Variable.Anesth Analg. 2020 Jul;131(1):e43. doi: 10.1213/ANE.0000000000004892. Anesth Analg. 2020. PMID: 32304464 Free PMC article. No abstract available.
-
Optimizing Clinical Staffing in Times of a Pandemic Crisis Such as COVID-19.Anesth Analg. 2020 Jul;131(1):e45-e47. doi: 10.1213/ANE.0000000000004903. Anesth Analg. 2020. PMID: 32332296 Free PMC article. No abstract available.
References
-
- Nizamuddin J, Tung A. Intensivist staffing and outcome in the ICU: daytime, nighttime, 24/7? Curr Opin Anaesthesiol. 2019;32:123–128. - PubMed
