

Liver-related mortality is similar among men and women with cirrhosis
- PMID: 32344052
- PMCID: PMC7572539
- DOI: 10.1016/j.jhep.2020.04.022
Liver-related mortality is similar among men and women with cirrhosis
Abstract
Background & aims: Sex-based differences are known to significantly contribute to outcomes in patients with chronic liver diseases; however, the role of patient sex in cirrhosis is unclear. We aimed to study the relationship between patient sex and cirrhosis.
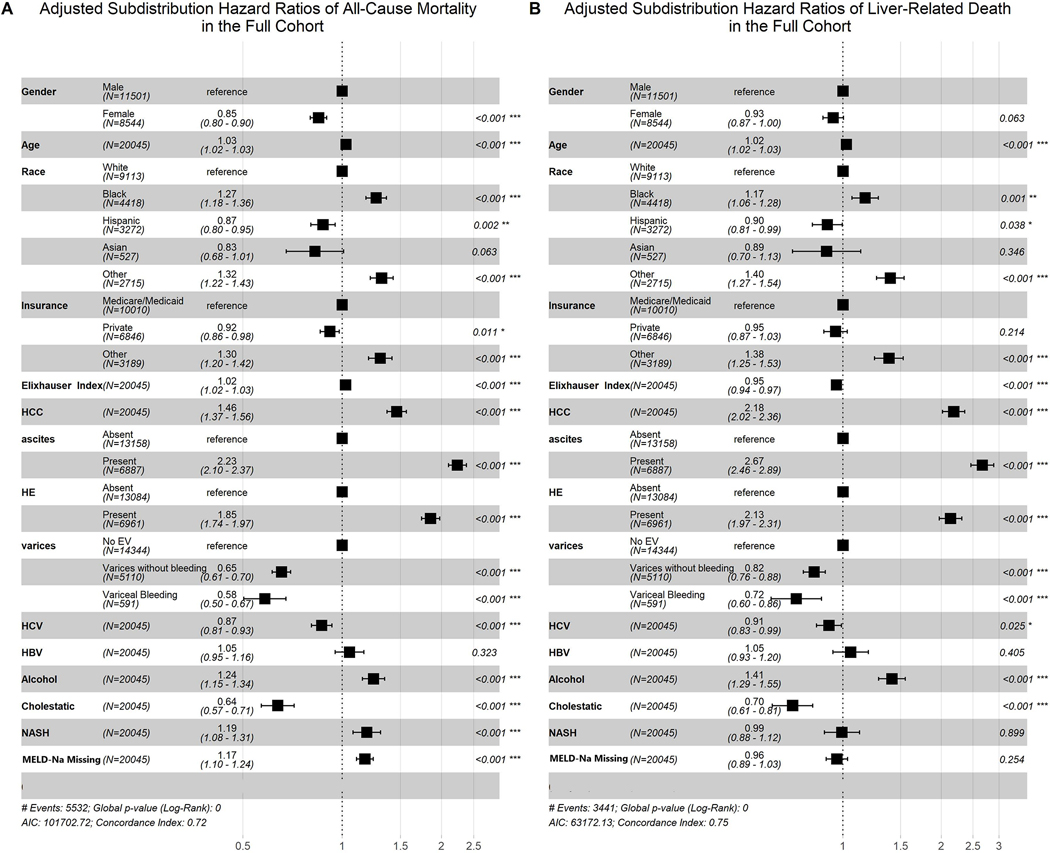
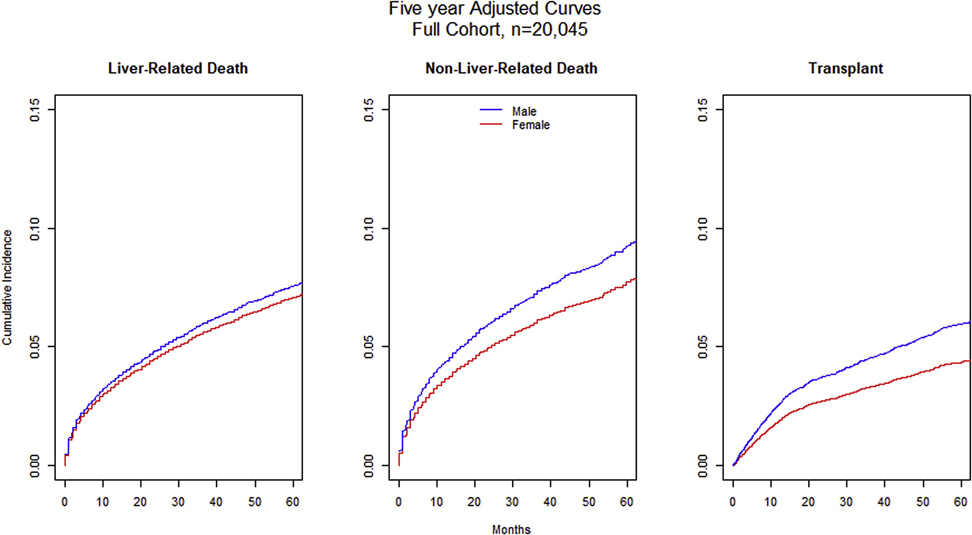
Methods: We analyzed a cohort of 20,045 patients with cirrhosis using a Chicago-wide electronic health record database that was linked with the United Network for Organ Sharing and cause of death data from the state death registry. Adjusted Cox survival analyses and competing risk analyses were performed to obtain subdistribution hazard ratios (HRs) for liver-related cause of death.
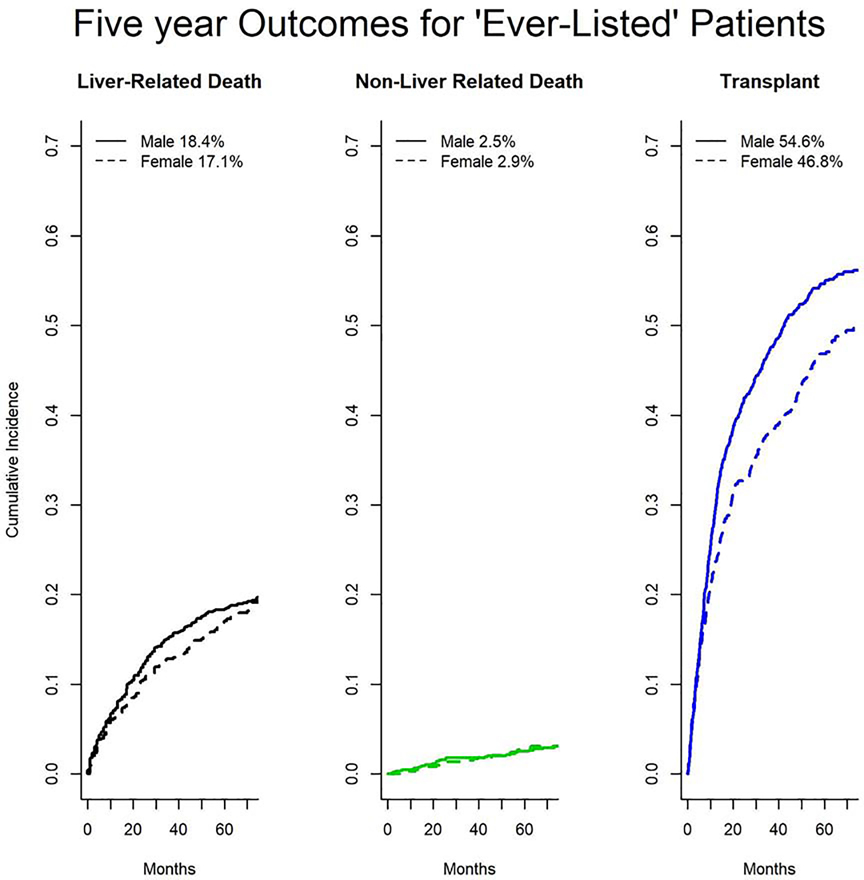
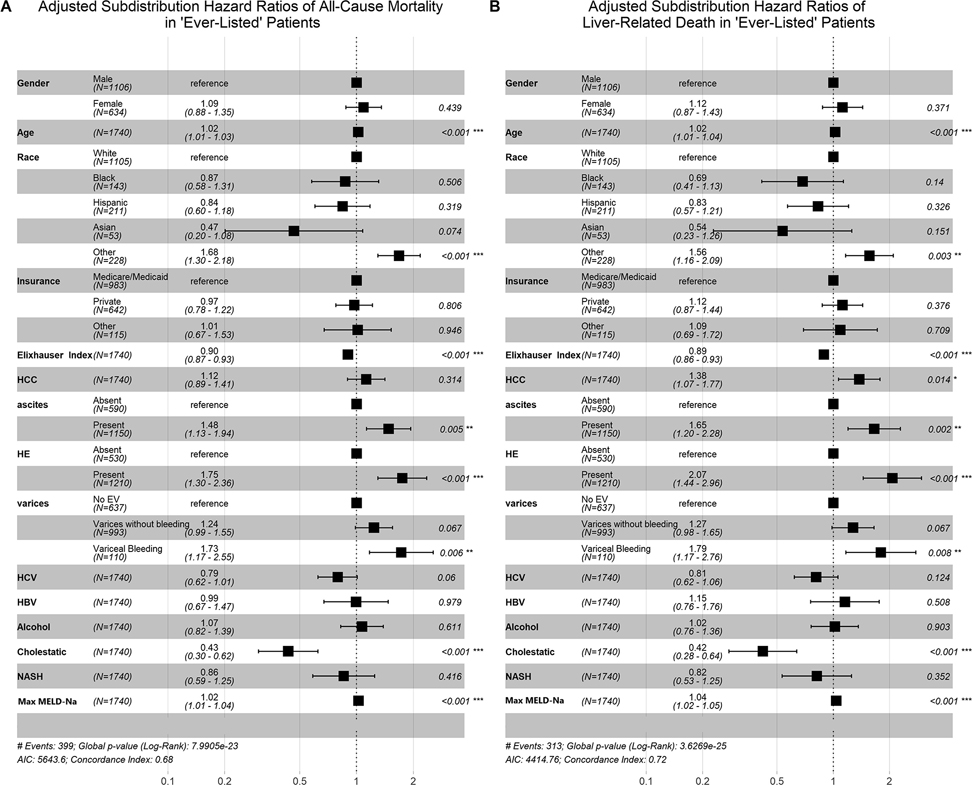
Results: Female and male patients had similar age, racial distribution, insurance status, and comorbidity status by Elixhauser score. Females had higher rates of cholestatic liver disease (17.1% vs. 6.2%, p <0.001) and non-alcoholic steatohepatitis (29.8% vs. 21.2%, p <0.001) than males. They were less likely to have portal hypertensive complications and had lower peak MELD-Na scores during follow-up. Female sex was associated with a decreased hazard of all-cause mortality (adjusted HR 0.85; 95% CI 0.80-0.90). This effect was attenuated when liver-related mortality was examined (subdistribution HR 0.93; 95% CI 0.87-1.00). No significant difference was noted for women who were 'ever-listed' in competing risk analyses for either all-cause mortality (subdistribution HR 1.09; 95% CI 0.88-1.35) or liver-related death (subdistribution HR 1.12; 95% CI 0.87-1.43), despite lower rates of listing (7.5% vs. 9.8%; p <0.001) and transplant (3.5% vs. 5.2%; p <0.001).
Conclusions: In this longitudinal study of patients with cirrhosis, female sex was associated with a survival advantage likely driven by lower rates of non-liver-related death. Women were not at an increased risk of liver-related death despite lower rates of listing and transplantation.
Lay summary: Patient sex is an important contributor in many chronic diseases, including cirrhosis. Prior studies have suggested that female sex is associated with worse outcomes. We analyzed a cohort of 20,045 patients with cirrhosis using a Chicago-wide electronic health record database. Using multivariate competing risk analyses, we found that female sex in cirrhosis is actually associated with a lower risk of all-cause mortality and has no association with liver-related mortality. Our findings are novel because we show that women with cirrhosis have a similar risk of liver-related death as their male counterparts, despite lower rates of listing and transplantation.
Keywords: Cirrhosis; Disparities; Female; Gender; Outcomes.
Copyright © 2020 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
References
-
- Murphy SL, Xu J, Kochanek KD, Curtin SC, Arias E. National Vital Statistics Reports Volume 66, Number 6, November 27, 2017. vol. 66. 2015. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
