

Serial CT analysis in idiopathic pulmonary fibrosis: comparison of visual features that determine patient outcome
- PMID: 32345689
- PMCID: PMC7402558
- DOI: 10.1136/thoraxjnl-2019-213865
Serial CT analysis in idiopathic pulmonary fibrosis: comparison of visual features that determine patient outcome
Abstract
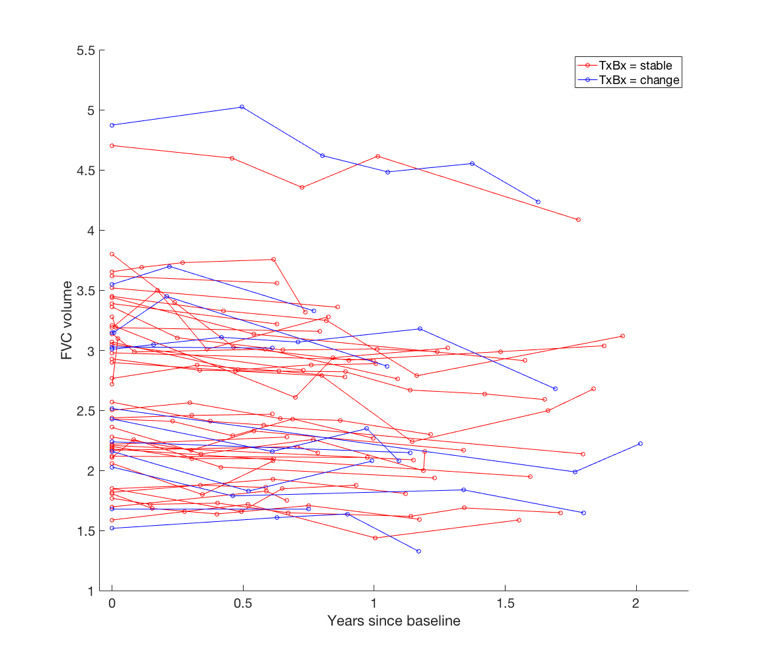
Aims: Patients with idiopathic pulmonary fibrosis (IPF) receiving antifibrotic medication and patients with non-IPF fibrosing lung disease often demonstrate rates of annualised forced vital capacity (FVC) decline within the range of measurement variation (5.0%-9.9%). We examined whether change in visual CT variables could help confirm whether marginal FVC declines represented genuine clinical deterioration rather than measurement noise.
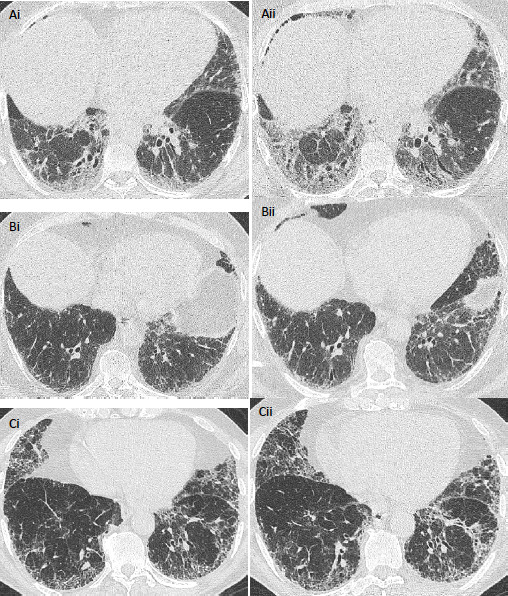
Methods: In two IPF cohorts (cohort 1: n=103, cohort 2: n=108), separate pairs of radiologists scored paired volumetric CTs (acquired between 6 and 24 months from baseline). Change in interstitial lung disease, honeycombing, reticulation, ground-glass opacity extents and traction bronchiectasis severity was evaluated using a 5-point scale, with mortality prediction analysed using univariable and multivariable Cox regression analyses. Both IPF populations were then combined to determine whether change in CT variables could predict mortality in patients with marginal FVC declines.
Results: On univariate analysis, change in all CT variables except ground-glass opacity predicted mortality in both cohorts. On multivariate analysis adjusted for patient age, gender, antifibrotic use and baseline disease severity (diffusing capacity for carbon monoxide), change in traction bronchiectasis severity predicted mortality independent of FVC decline. Change in traction bronchiectasis severity demonstrated good interobserver agreement among both scorer pairs. Across all study patients with marginal FVC declines, change in traction bronchiectasis severity independently predicted mortality and identified more patients with deterioration than change in honeycombing extent.
Conclusions: Change in traction bronchiectasis severity is a measure of disease progression that could be used to help resolve the clinical importance of marginal FVC declines.
Keywords: bronchiectasis; idiopathic pulmonary fibrosis; imaging/CT.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: JJ reports personal fees from Boehringer Ingelheim outside the current work. AUW reports personal fees from Intermune, Boehringer Ingelheim, Gilead, MSD, Roche, Bayer and Chiesi outside the submitted work. SRD reports personal fees from Boehringer Ingelheim outside the submitted work. Work by CHMM, HWE, FTB and MV was supported by ZonMW TopZorg Care (grant number 842002001).
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials