

Emergency department use by pregnant women in Ontario: a retrospective population-based cohort study
- PMID: 32345709
- PMCID: PMC7207029
- DOI: 10.9778/cmajo.20190154
Emergency department use by pregnant women in Ontario: a retrospective population-based cohort study
Abstract
Background: Peripregnancy emergency department use may be common, but data specific to health care systems like that in Canada are lacking. As prior research was limited to livebirths, omitting pregnancies ending in miscarriage or induced abortion, the current study quantified and characterized emergency department use among women in Ontario with a recognized pregnancy.
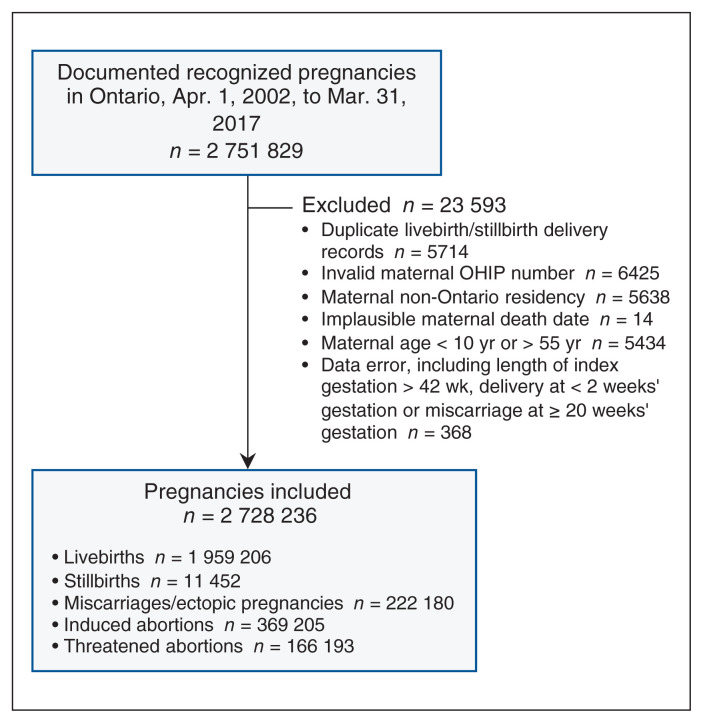
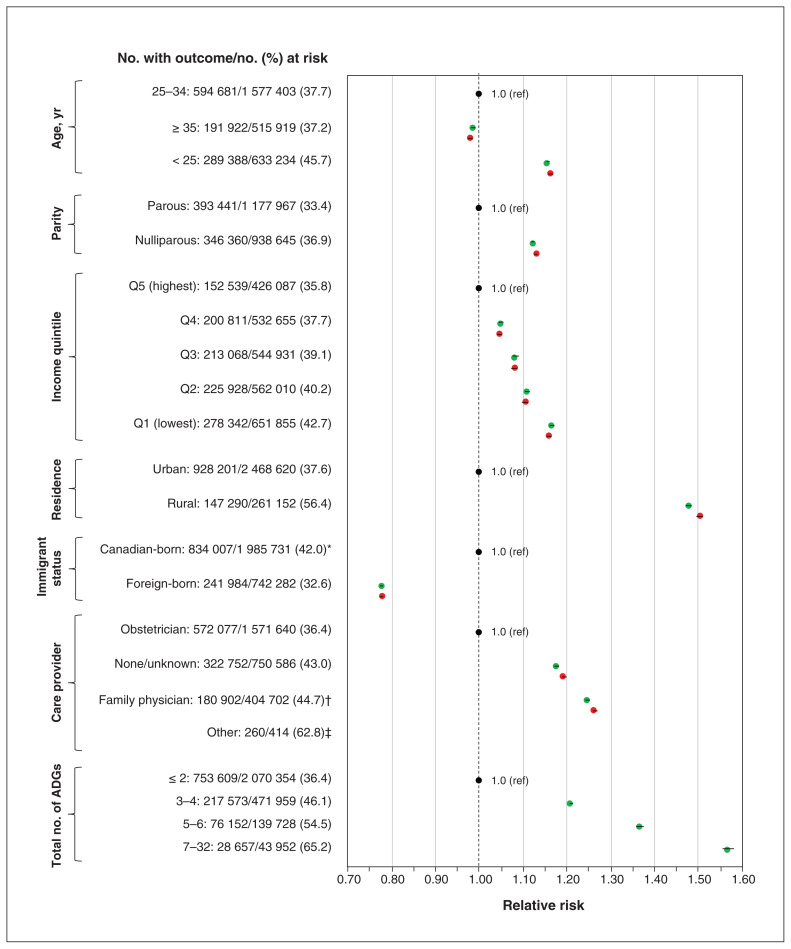
Methods: This retrospective population-based cohort study included all recognized pregnancies among Ontario residents aged 10-55 years with an estimated date of conception between Apr. 1, 2002, and Mar. 31, 2017. We defined peripregnancy emergency department use as any emergency department visit during pregnancy or within 42 days after pregnancy. We used modified Poisson regression with a robust error variance to generate relative risks (RRs) and 95% confidence intervals (CIs) for the outcome of any peripregnancy emergency department use in association with maternal age, parity, residential income quintile, location of residence, immigrant status, antenatal care provider and number of comorbidities within 120 days before the clinical start of the pregnancy (expressed as total number of Aggregated Diagnosis Groups [ADGs] obtained with the Johns Hopkins Adjusted Clinical Group System). All RRs, except for number of comorbidities, were further adjusted for number of ADGs.
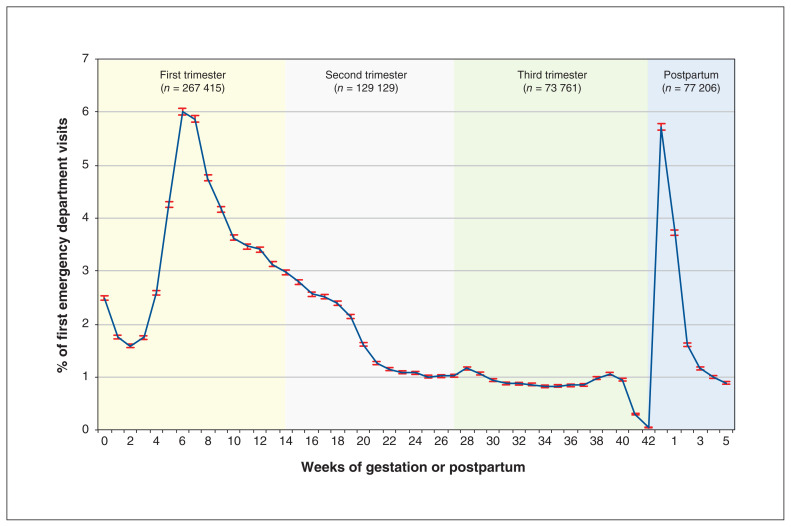
Results: Peripregnancy emergency department use occurred in 1 075 991 (39.4%) of 2 728 236 recognized pregnancies, including 35.8% of livebirths, 47.3% of stillbirths, 73.7% of miscarriages and 84.8% of threatened abortions. A peripregnancy emergency department visit was more likely among women who were less than 25 years of age (adjusted RR 1.16, 95% CI 1.16-1.17), were nulliparous (adjusted RR 1.13, 95% CI 1.13-1.13), resided in the lowest income quintile area (adjusted RR 1.16, 95% CI 1.15-1.16) or in a rural area (adjusted RR 1.50, 95% CI 1.50-1.51), were Canadian-born (adjusted RR 1.22, 95% CI 1.22-1.23), were not seen by an obstetrician (adjusted RR 1.66, 95% CI 1.54-1.80) or had a greater number of ADGs. Emergency department use peaked in the first trimester and in the first week postpartum. Compared to women residing in urban areas, those residing in rural areas had an odds ratio (OR) of 3.44 (95% CI 3.39-3.49) for 3 or more emergency department visits. Women with 3-4 (OR 1.99, 95% CI 1.97-2.01), 5-6 (OR 3.55, 95% CI 3.49-3.61), or 7 or more (OR 7.59, 95% CI 7.39-7.78) prepregnancy comorbidities were more likely to have 3 or more peripregnancy emergency department visits than were those with 2 or fewer comorbidities.
Interpretation: Peripregnancy emergency department use occurred in nearly 40% of pregnancies, notably in the first trimester and early in the postpartum period. Efforts are needed to streamline rapid access to ambulatory obstetric care during these peak periods, when women are susceptible to miscarriage or a complication after a livebirth.
Copyright 2020, Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Malik S, Kothari C, MacCallum C, et al. Emergency department use in the perinatal period: an opportunity for early intervention. Ann Emerg Med. 2017;70:835–9. - PubMed
-
- Cunningham SD, Magriples U, Thomas JL, et al. Association between maternal comorbidities and emergency department use among a national sample of commercially insured pregnant women. Acad Emerg Med. 2017;24:940–7. - PubMed
-
- Vladutiu CJ, Stringer EM, Kandasamy V, et al. Emergency care utilization among pregnant Medicaid recipients in North Carolina: an analysis using linked claims and birth records. Matern Child Health J. 2019;23:265–76. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous