

Feasibility of blood testing combined with PET-CT to screen for cancer and guide intervention
- PMID: 32345712
- PMCID: PMC7509949
- DOI: 10.1126/science.abb9601
Feasibility of blood testing combined with PET-CT to screen for cancer and guide intervention
Abstract
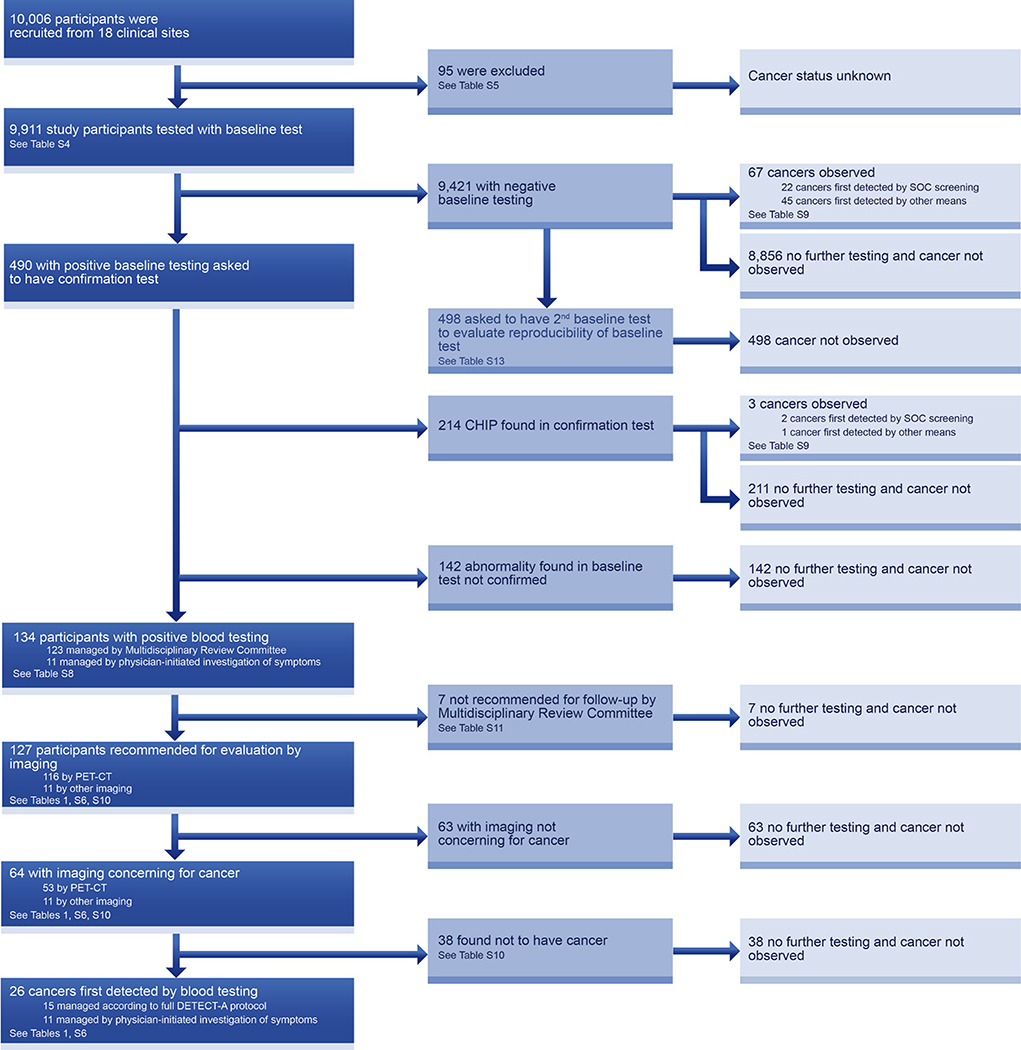
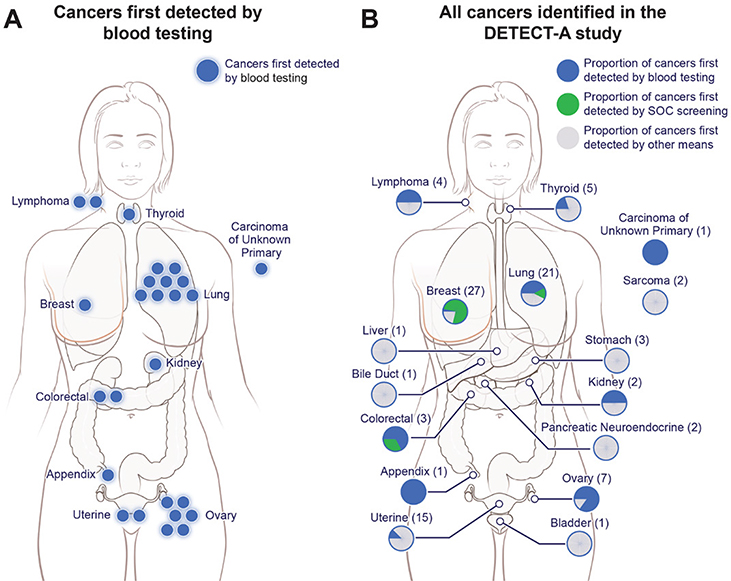
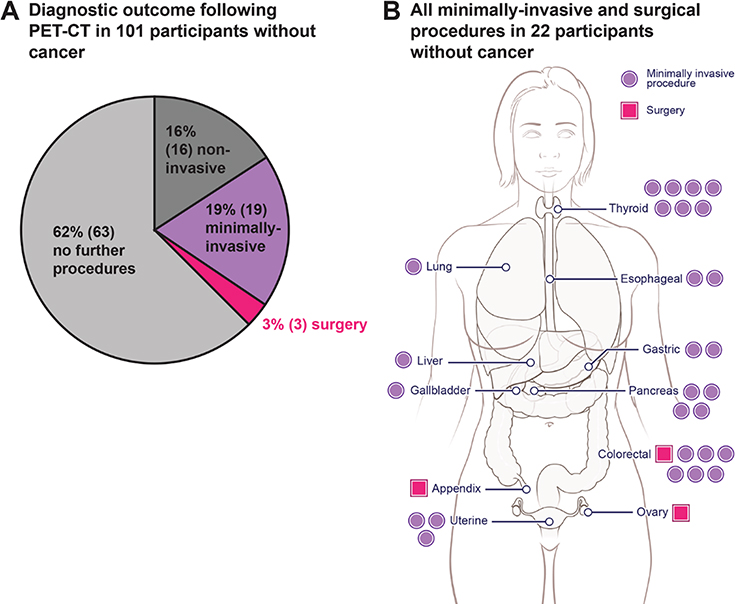
Cancer treatments are often more successful when the disease is detected early. We evaluated the feasibility and safety of multicancer blood testing coupled with positron emission tomography-computed tomography (PET-CT) imaging to detect cancer in a prospective, interventional study of 10,006 women not previously known to have cancer. Positive blood tests were independently confirmed by a diagnostic PET-CT, which also localized the cancer. Twenty-six cancers were detected by blood testing. Of these, 15 underwent PET-CT imaging and nine (60%) were surgically excised. Twenty-four additional cancers were detected by standard-of-care screening and 46 by neither approach. One percent of participants underwent PET-CT imaging based on false-positive blood tests, and 0.22% underwent a futile invasive diagnostic procedure. These data demonstrate that multicancer blood testing combined with PET-CT can be safely incorporated into routine clinical care, in some cases leading to surgery with intent to cure.
Copyright © 2020, American Association for the Advancement of Science.
Conflict of interest statement
Figures

Comment in
-
Pan-Cancer Early Detection: Hype or Hope?Cancer Cell. 2020 Jul 13;38(1):23-24. doi: 10.1016/j.ccell.2020.05.021. Epub 2020 Jun 11. Cancer Cell. 2020. PMID: 32531269
-
Multi-cancer blood testing combined with PET-CT: road for hope to screen for cancer and guide intervention.Signal Transduct Target Ther. 2020 Jun 12;5(1):95. doi: 10.1038/s41392-020-0210-2. Signal Transduct Target Ther. 2020. PMID: 32532963 Free PMC article. No abstract available.
-
Towards multi-cancer screening using liquid biopsies.Nat Rev Clin Oncol. 2020 Sep;17(9):525-526. doi: 10.1038/s41571-020-0404-0. Nat Rev Clin Oncol. 2020. PMID: 32555396 No abstract available.
-
Combining liquid biopsies and PET-CT for early cancer detection.Nat Med. 2020 Jul;26(7):1010-1011. doi: 10.1038/s41591-020-0970-9. Nat Med. 2020. PMID: 32601339 No abstract available.
References
-
- Howlader N et al., Eds., SEER Cancer Statistics Review, 1975–2014, National Cancer Institute, Bethesda, MD: (2017).
-
- Goldblum JR, Lamps LW, McKenney J, Myers JL, Surgical Pathology. (Elsevier, 2018).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
